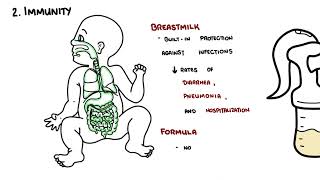
Hyperemesis gravidarum (HG) exists on a spectrum of nausea and vomiting in pregnancy (NVP). NVP refers to symptoms of nausea, vomiting or dry retching commencing in the first trimester, with no other cause identified.1 HG refers to severe, persistent vomiting that may result in malnutrition, dehydration, weight loss and debility due to illness. HG is a serious illness of pregnancy and may lead to fatality.2
Hyperemesis gravidarum affects ~10% of pregnancies and recurs in up to 80% of future pregnancies. With timely management, maternal prognosis is good and long-term complications are rare. Without treatment, HG can progress to severe complications including nutritional deficiency, refeeding syndrome, Wernicke’s encephalopathy, and even death. Adverse fetal outcomes include growth restriction, placental abruption, pre-eclampsia, and potential long-term neurodevelopmental delay.
Definition
Hyperemesis gravidarum: Severe, persistent nausea and vomiting in pregnancy, usually in the first trimester, leading to weight loss (>5% pre-pregnancy weight), dehydration, electrolyte imbalance, and ketonuria. Common morning sickness is milder and does not usually affect hydration or nutrition. hCG: human chorionic gonadotropin. A hormone produced by the placenta during pregnancy. Wernicke’s encephalopathy: sudden, severe neurological disorder caused by deficiency of thiamine.
Anatomy/ Physiology
Nausea
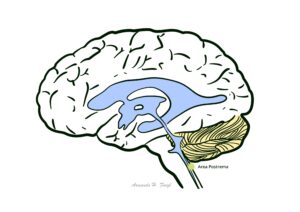
The sensation of nausea is thought to arise differently to vomiting, however is poorly understood. It is thought to arise through the activation of higher brain centres, as well as the involvement of the medulla oblongata, which is involved in creating a conscious feeling of nausea. One recently studied area is the area postrema within the medulla oblongata, which activates the perception of nausea and vomiting.4,5
This image series is only available to members
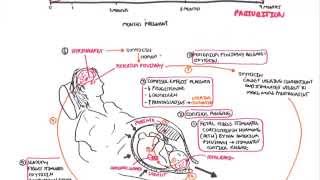
Summary of Vomiting Mechanism
Gut–brain axis: Vomiting is coordinated by the brain (vomiting centre and CTZ) and the gut.
Vomiting centre: Located in the medulla oblongata; contains muscarinic receptors. Activation of these receptors directly initiates vomiting.
Chemoreceptor trigger zone (CTZ): Also in the medulla but outside the blood–brain barrier, making it sensitive to circulating drugs and toxins. Contains dopamine and serotonin receptors. Stimulation of the CTZ activates the vomiting centre.
Gut/stomach: Enterochromaffin cells in the gastric mucosa release serotonin, which stimulates 5HT3 receptors on vagal sensory nerves. These signals travel to the vomiting centre.
Vomiting reflex: Once triggered, the lower oesophageal sphincter relaxes, diaphragm and abdominal muscles contract, and autonomic changes occur (tachycardia, salivation, increased peristalsis), resulting in expulsion of gastric contents.
Though complex, the main process of vomiting surrounds the vomiting centre which gets input from the CTZ, the gut and higher cortical centres.
Aetiology and Risk Factors
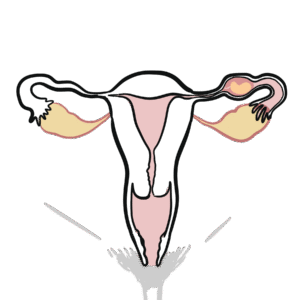
History of HG in previous pregnancies, multiple pregnancy, younger maternal age
High recurrence risk → anticipate early in future pregnancies.
Pathophysiology
The pathophysiology of NVP and HG remains incompletely understood, but is thought to involve a combination of genetic, hormonal, and environmental factors.
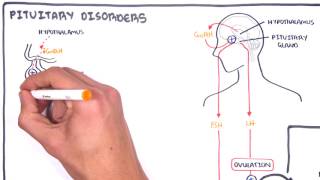
Increased GDF15: growth/differentiation factor
GDF15, a member of the TGF-β family, is produced by the placenta, as well as the prostate and abdominal viscera.
In the brain, it acts via GFRAL receptors located in the area postrema (see anatomy/physiology).
During pregnancy, stressors such as nutritional stress increase GDF15, → activating GFRAL receptors → contributes to nausea and vomiting.
It is found that patients admitted for HG have higher levels of GDF15 than pregnant patients without HG.
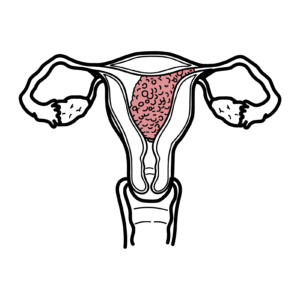
Increased hCG
The peak of hCG production correlates with the peak of NVP and HG — 12-14 weeks gestation. Further, NVP is worse in pregnant women who endure conditions with increased hCG levels including molar pregnancy, Down’s syndrome and multiple gestations.
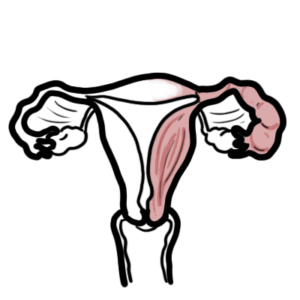
Estrogen and progesterone
It is postulated that estrogen contributes to HG through nitric oxide production → relaxing smooth muscle in the gut, slowing intestinal transit time and gastric emptying → increasing nausea and vomiting. Progesterone further decreases smooth muscle contractility of the stomach, slowing gastric emptying.
HG is likely related to hCG & estrogen stimulation of the chemoreceptor trigger zone.
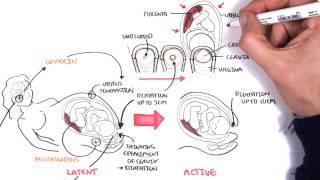
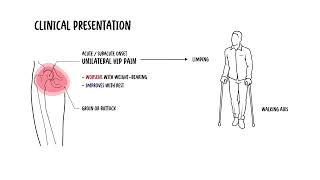
Clinical manifestation
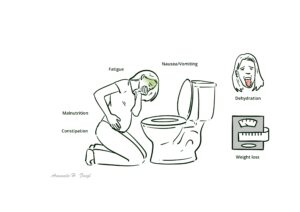
Continuous nausea and vomiting
Generally beginning 6 weeks gestation, resolving 16-20 weeks gestations. Though, in 20% of cases, nausea and vomiting persist through entire pregnancy
Inability to maintain adequate oral intake of food and fluid
Fatigue with inability to perform daily activities
SEVERE: malnutrition
Malnutrition may result in electrolyte imbalance as well as vitamin/mineral deficiencies that may cause significant complications such as Wernicke’s encephalopathy
This image series is only available to members
Assess for signs of complications of hyperemesis gravidarum as they need to be treated promptly.
Diagnosis
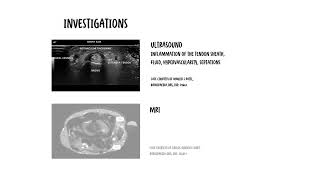
Investigations performed for hyperemesis gravidarum are dependent on its severity. Investigations ordered may include
UECs: electrolyte imbalance, signs of AKI due to dehydration
For alternate diagnoses: TFTs, lipase, urine MCS, LFTs
Coagulation studies
Two tools exist to determine the diagnosis and management of HG.
PUQE-24 is a validated tool to assess the severity of nausea and vomiting. It consists of a questionnaire which is filled out by patients, as outlined below7:
PUQE-24
Question
Response Options
Score
1. In the last 24 hours, for how long have you felt nauseated or sick to your stomach?
Not at all (1) 1 hour or less (2) 2–3 hours (3) 4–6 hours (4) More than 6 hours (5)
1–5
2. In the last 24 hours, have you vomited or thrown up?
I did not vomit (1) 1–2 times (2) 3–4 times (3) 5–6 times (4) 7 or more times (5)
1–5
3. In the last 24 hours, how many times have you had retching or dry heaves without throwing up?
None (1) 1–2 times (2) 3–4 times (3) 5–6 times (4) 7 or more times (5)
1–5
Interpreting the total score4 – 6: mild NVP7 – 12: moderate NVP≥13: HG
The HELP score, developed by the HER (Hyperemesis Education and Research) Foundation, is a more comprehensive assessment tool that can guide the treatment of a patient’s nausea and vomiting, or hyperemesis gravidarum.
As nausea and vomiting is a non-specific finding, differential diagnoses are broad in nature. A systems-based approach will assist in ruling out differentials.
It is crucial to assess for differentials if the onset of nausea and vomiting is later than the expected onset of NVP (around 6 weeks of gestation) as it is a higher likelihood to be nausea and vomiting associated with a different cause.
Always exclude molar pregnancy.
Treatment
Mild HG
Pyridoxine and doxylamine
Pyridoxine: 12.5mg PO morning, midday. 25mg at night
Doxylamine: 25mg PO nocte
If not effective, add any of the following: PRN
Metoclopramide: 10mg PO, 8 hourly
Ondansetron: 4-8mg PO, 10-12 hourly
Prochlorperazine: 5-10mg PO, 6-8 hourly
Promethazine: 10-25mg PO, 6-8 hourly
Severe HG: any of the following PRN:
Metoclopramide: 10mg IV/IM, 8 hourly
Ondansetron: 4-8mg IV, 8-12 hrly
Prochlorperazine: 12.5mg IM or slow IV injection, 8 hourly
With appropriate management, maternal prognosis from HG is favourable, with no known long-term complications. Without appropriate interventions, mild to life-threatening complications can occur (see above). In terms of foetal prognosis, long-term complications are under research. Emerging evidence suggests that offspring may exhibit neurodevelopmental (e.g., ADHD, ASD) and psychological disorders, though more research is required.
References
Lowe SA, Bowyer L, Beech A, Robinson H, Armstrong G, Marnoch C, Grzeskowiak L. Guideline for the management of nausea and vomiting in pregnancy and hyperemesis gravidarum. SOMANZ; 2019.
Vadakekut ES, Mahdy H. Hyperemesis Gravidarum.Treasure Island (FL): StatPearls Publishing; 2025.
Hyperemesis Education and Research [HER] Foundation. HER Hyperemesis Gravidarum Facts. 2023. Accessed September 05, 2025
Lee NM, Saha S. Nausea and vomiting of pregnancy. Gastroenterol Clin North Am. 2011;40(2):309-34, vii. doi: 10.1016/j.gtc.2011.03.009.
Liu C, Zhao G, Qiao D, Wang L, He Y, Zhao M, Fan Y, Jiang E. Emerging Progress in Nausea and Vomiting of Pregnancy and Hyperemesis Gravidarum: Challenges and Opportunities. Front Med (Lausanne). 2022;8:809270. doi: 10.3389/fmed.2021.809270.










Discussion