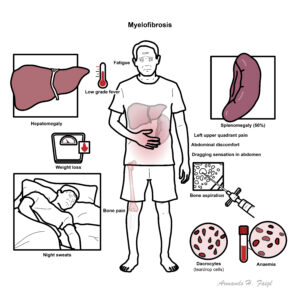
Myelofibrosis


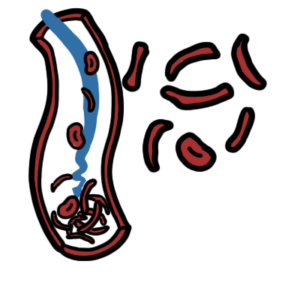
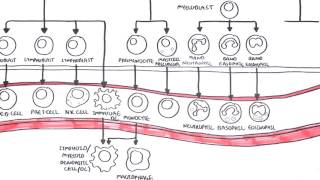
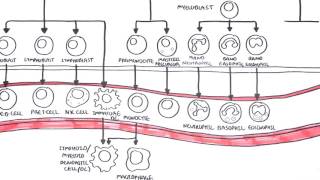
Myelofibrosis is a type of myeloproliferative diseasecharacterized by clonal myeloid expansion, followed by progressive fibrous connective tissue deposition in the bone marrow, resulting in bone marrow failure. Clonal evolution can also occur, with an increased risk of transformation to acute myeloid leukemia. In addition, disabling constitutional symptoms secondary to the high circulating levels of proinflammatory cytokines and hepatosplenomegaly frequently impair quality of life.
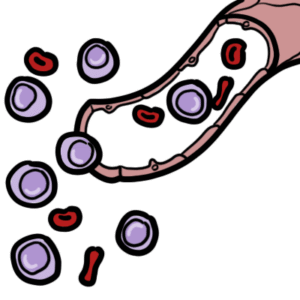
Myeloproliferative disorder: are clonal stem disorders characterised by leukocytosis, thromboytosis, erythrocytosis, splenomegaly, and bone marrow hypercelluarity. Includes myelofibrosis, essential thrombocytopaenia and polycythaemia
Primary Myelofibrosis: one of the chronic myeloproliferative disorders, where there is replacement of bone marrow with collagenous connective tissue and progressive fibrosis
Secondary Myelofibrosis: Myelofibrosis caused secondary to another disease such as essential thrombocytopnaeia or polycythaemia rubra vera
Essential Thrombocytopaenia: one of the chronic myeloproliferative disorders, in which too many platelets are produced in the bone marrow
Polycythaemia rubra vera: one of the chronic myeloproliferative disorders, which are collectively characterized by clonal proliferation of myeloid cells with variable morphologic maturity and hematopoietic efficiency.
Three main types of myeloproliferative disorders are PRV, ET and PMF.
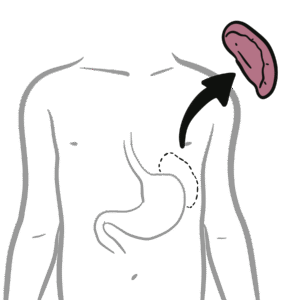
Hypersplenism triad: splenomegaly, pancytopenia and normocellular bone marrow.
Exact mechanism of disease is unknown but factors include:
General
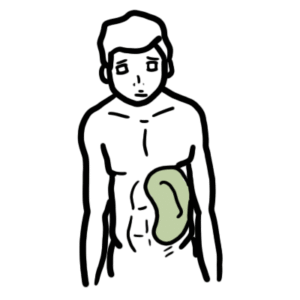
Symptoms of splenomegaly (50% of cases)
Symptoms of hypermetabolic state
Sites and signs and symptoms of extramedullary haematopoesis
Other tests
Diagnosis The 2008 WHO criteria include a combination of the following findings:
| MAJOR CAUSES OF SPLENOMEGALY | |
| Aetiology | Conditions |
| Congestion | Cirrhosis, Heart Failure, Thrombosis of portal/hepatic/splenic vein |
| Malignancy | Lymphoma, Leukaemia, Myeloproliferative disorders, Primary or secondary tumour |
| Infection | Viral (hepatitis, infectious mononucleosis, cytomegalovirus), bacterial (Salmonella, TB), parasitic (malaria, toxoplasmosis, schistosomiasis), infective endocarditis |
| Inflammation | Sarcoids, SLE, Rheumatoid arthritis (Felty syndrome) |
| Infiltrative, nonmalignant | Gacuher’s disease, Niemann-pick disease, Amyloid, Langerhan cell histiocytosis |
| Haematologic (hypersplenic) states | Haemolytic anaemias, Sick cell disease (children) |
More information on the differential diagnosis of Splenomegaly.
No direct relation between splenic size and hypersplenism, however hypersplenism is more common among those who have gross splenomegaly.
Hypersplenism is a triad of splenomegaly, pancytopenia and normocellular bone marrow. Splenomegaly increases the spleen’s mechanical filtering and destruction of RBCs and often of WBCs and platelets. Compensatory bone marrow hyperplasia occurs in those cell lines that are reduced in the circulation.
Overview
The initial management of patients with PMF is largely dictated by the risk of disease progression and estimated overall survival as calculated by prognostic scores
Asymptomatic (30% of patients)
Symptomatic
Bone marrow transplant offers the only currative potential for patients with PMF, however only a selected few will be able to have this.
Interferon therapy can be limited by its induction of leukopenia or thrombocytopenia, but it can decrease splenomegaly. This is particularly useful in pregnancy where chemotherapy and thalidomide are contraindicated.
Ruxolitinib is a JAK2 inhibitor used to treat myeloproliferative disorders. JAK2 (and other kinases) are responsible for the mediation of cytokine and growth factor signalling which in turn effect immune function and hematopoiesis. Side effects anemia, equilibrium disturbance, labyrinthitis, meniere’s disease, dizziness, headache, vertigo, neutropenia, thrombocytopenia, orthostatic dizziness, weight gain and flatulence. No contraindications.
Danazol is a synthetic steroid (androgen) with antigonadotropic and anti-estrogenic activities that acts as an anterior pituitary suppressant by inhibiting the pituitary output of gonadotropins. Danazol is usually used to treat endometriosis and fibrocystic breast disease (in patients unresponsive to simple measures). Also used for the prophylactic treatment of all types of hereditary angioedema in males and females. Danazol has been shown to stimulate erythropoiesis in patients with refractory anemia, leading to increased Hb level, reticulocytosis, and decreased need for blood transfusions. Side effects of androgen therapy include fluid retention, increased libido, hirsutism, abnormal liver function tests, and hepatic tumors.
Management post Splenectomy
Primary myelofibrosis has a median lifespain of ~5.5 years. Death is usually a consequence of bone marrow failure (haemorrhage, anaemia, or infection), transformation to acute leukaemia, portal HTN, heart failure, cachexia, or myeloid metaplasia with organ failure.











Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion