Bronchiolitis is often a viral cause mainly Respiratory Syncytial Virus (RSV). Bronchiolitis is the most common respiratory tract infection of neonates and is usually self-limiting. A major source of confusion of treatment is differentiating a viral bronchiolitis to asthma. In summary bronchiolitis is usually seen in infants <2yo. Asthma is seen in older children.
Exclusive breastfeeding for at least 6 months is recommended to decrease the morbidity of respiratory infections.
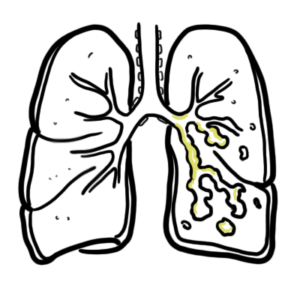
Pathophysiology
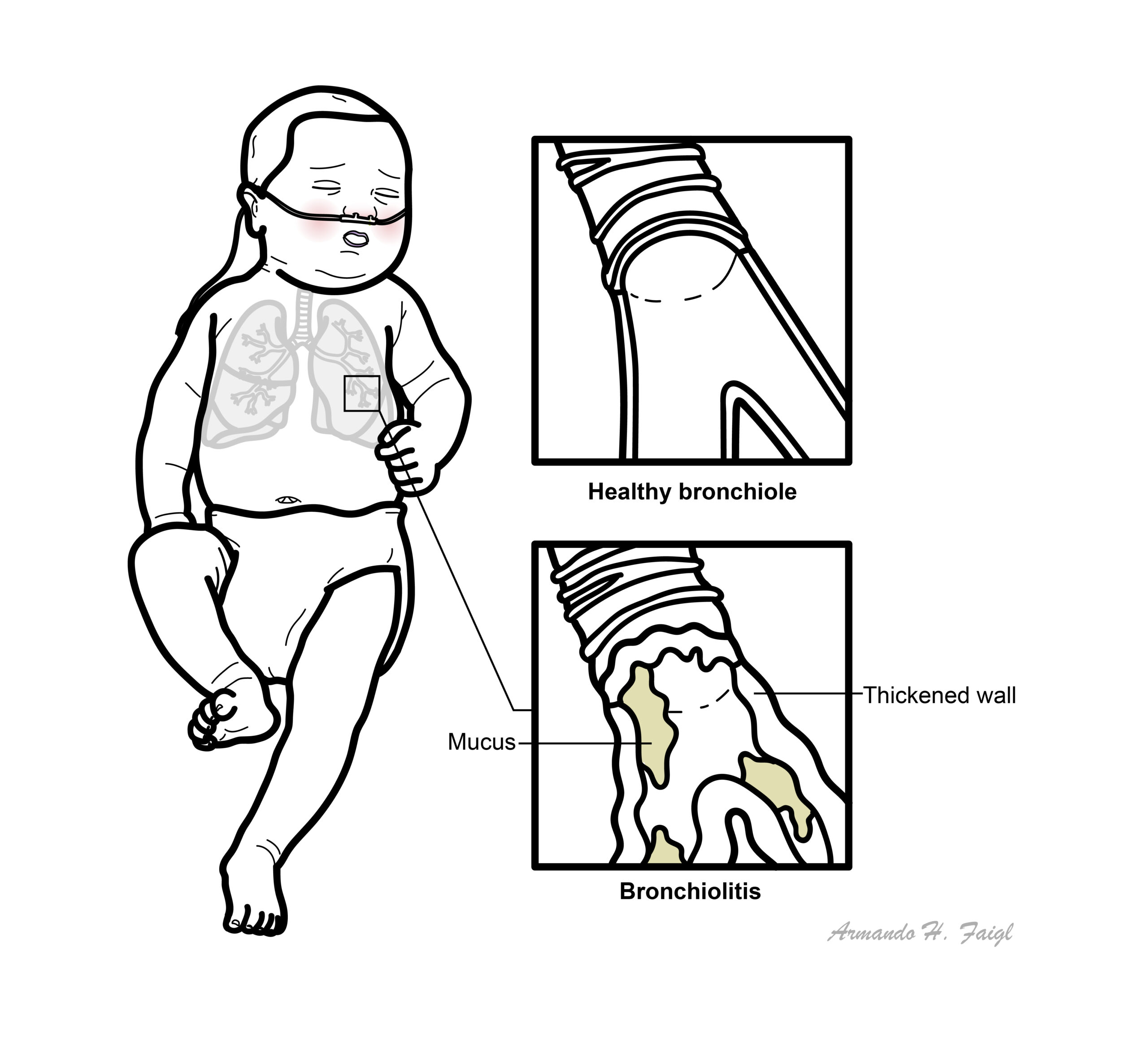
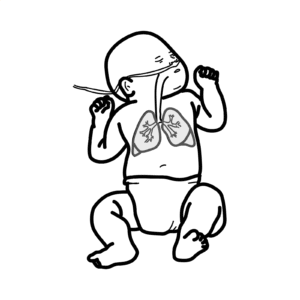
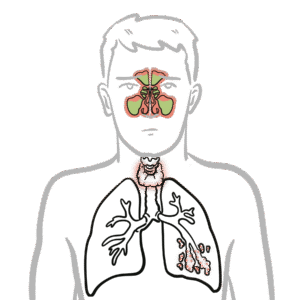
An RSV infection begins with replication of the virus in the nasopharynx. The virus spreads to the small bronchiolar epithelium lining the small airways within the lungs, and a lower respiratory tract infection can begin in one to three days. If a lower respiratory tract infection occurs, it causes edema, increased mucus production, and eventual necrosis and regeneration of these epithelial cells. This leads to small airway obstruction, air trapping, and increased airway resistance.
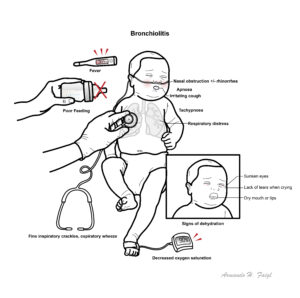
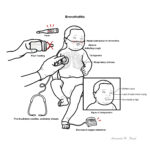
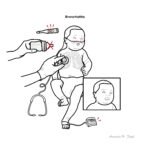
Clinical Presentation Nasal obstruction +/- rhinorrhea and an irritating cough are usually noticed first. After one to three days there follows increasing tachypnoea and respiratory distress. The chest is often overexpanded.
Increased work of breathing, chest wall retraction, nasal flaring
Decreased feeding
SaO2 90-95%
Severe bronchiolitis
Usually require transfer to a tertiary paediatric ICU
Moderate to serve respiratory distress, with marked chest wall retraction, nasal flaring and grunting
Very poor feeding, feeding may worsen the cough, tachycardia
Fluids
Oral feeding OR
Nasogastric tube for infants with poor feeding OR
Intravenous fluids if previous do not work and if infant have severe bronchiolitis
Pharmacological Therapy
Generally no bronchodilators <6months of age
Corticosteroids or ipratropium only in older infants, if asthma is considered, or infants with chronic lung disease
Antibiotics if bacterial cause is suspected
Bronchodilators (albuterol, salbutamol), epinephrine, and corticosteroids are generally not administered to infants and children with the diagnosis of bronchiolitis. Only if another condition is suspected or person is not getting better.
Discharge
Minimal respiratory distress
During the recovery phase, SaO2 92 or above room air
40 percent of children with bronchiolitis will develop further wheezing episodes through five years of age, and 10 percent will have wheezing episodes beyond this age.
References
Caswell, MD & Muncie, HL 2011, Repiratory Syncytial Virus Infection in Children, American Family Physician, vol. 15, no. 2, pp 141-146.
Ralston, SL, Lieberthal, AS, Meissner, HC, et al. 2014, Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis, vol. 123, no. 5.
Royal Children Hospital Melbourne Clinical Guidelines












Discussion