Peptic Ulcer Disease


Peptic ulcer refers to an ulcer in the lower oesophagus, stomach or duodenum. Incidence ↑ with age; both sexes are similarly affected. In the developed world, Helicobacter pylori incidence has been slowly ↓ over the past 50 yrs; Non-Steroidal Anti-Inflammatory drug (NSAID) use has ↑. Peptic ulcers remain common worldwide, especially in the developing world where H. pylori infection is prevalent.
Dyspepsia: “indigestion”; describes symptoms such as bloating & nausea, thought to originate from the upper GIT; a chronic or recurrent abdominal pain or discomfort centered in the upper abdomen
Ulcer: breach/ defect in mucosal lining of the stomach or duodenum that extends through the muscularis mucosae into the submucosa or deeper
Erosions: breech in epithelium of the mucosa only; do not penetrate muscularis mucosae
Metaplasia: a change in phenotype of differentiated cells in which one cell type is replaced by another cell type; may result in reduced functions or increased propensity for malignant transformation.
The stomach is a J-shaped organ located inferior to the diaphragm within the abdominal cavity. Stomach has three main function:
The lower esophageal sphincter and pyloric sphincter separates the stomach from the oesophagus and duodenum respectively. The parts of the stomach include:
Layers of the stomach
The inside of the stomach looks tortuous (Rugae) and forms gastric pits which contain many cells.
The stomach have a number of specialised cells that perform varies function
Intrinsic factor is needed for Vitamin B12 absorption.
Peptic ulcers result from an imbalance between factors:
Clinical Presentation
3 notable characteristics: localization to the epigastrium, relationship to food, episodic occurrence.
Examination
Medical Emergency – Perforated Ulcer
H. Pylori infection has reduced. This result in ↓ duodenal ulcers (almost always assoc with H. pylori infection) and ↑ in gastric ulcers (main site of ulcers caused by NSAIDs).
Medical management (mainstay of treatment, unless complicated)
H. pylori eradication:
Cornerstone of therapy for peptic ulcers as this will prevent relapse & eliminate
need for long-term therapy in the majority of patients
Triple therapy: PPI taken with 2 antibiotics (clarithromycin, amoxycillin or metronidazole) for 14 days
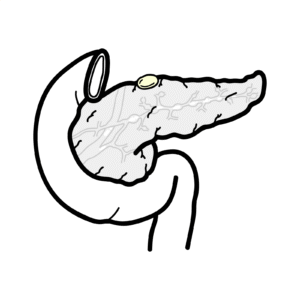
Peptic ulcer penetration occurs when chronic ulcer penetrates the entire thickness of the stomach or duodenal wall, into an adjacent organ such as the pancreas, but without free perforation into the peritoneal cavity.
Overview
Perforated Peptic ulcer is a surgical emergency. It is caused by erosion of the ulcer through the wall of the stomach or duodenum into the peritoneal cavity. The contents of the stomach escape into the peritoneal cavity → peritonitis (board-like rigidity). The commonest site of perforation is the anterior aspect of duodenum from a duodenal ulcer.
Clinical Presentation
Investigation
Management – Surgical Emergency
A Colour Handbook of Gastroenterology
Oxford Clinical Handbook of Clinical Medicine
Sleisenger and Fordtran’s Gastrointestinal and Liver Disease 10th Ed.











Discussion