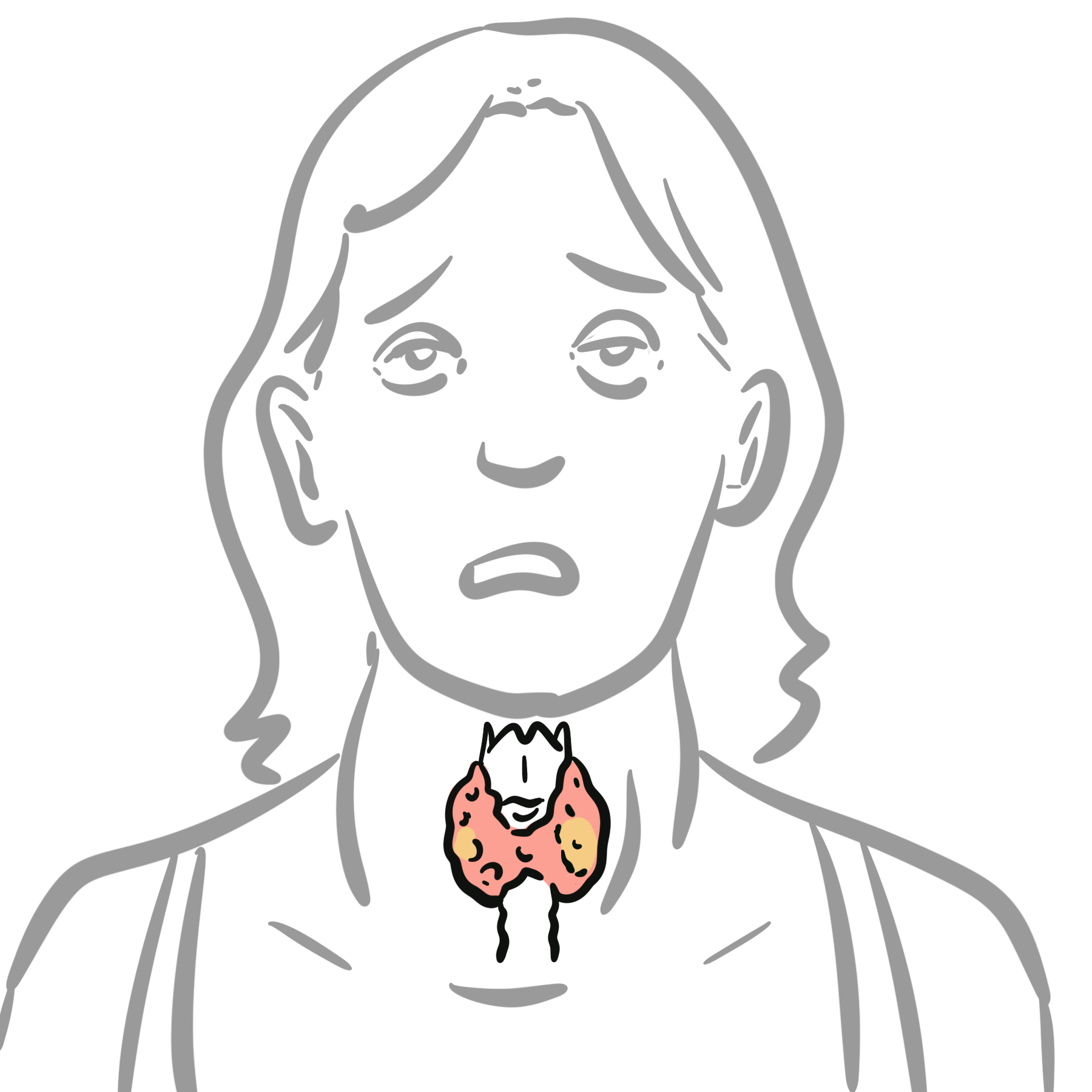
Toxic Multinodular Goitre (TMNG) is the second most common cause of hyperthyroidism caused by a long-standing goitre and/or iodine deficiency which results in an increased risk of mutation and consequent TSH-independent autonomic function of thyroid nodules to produce excess thyroid hormones. Common clinical manifestations include hyperthyroidism and a painless thyroid goitre with palpable nodules. The disease can be addressed and treated early on, with a good prognosis and clinical outcomes.
Definition
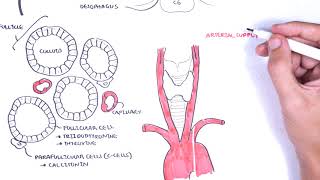
Goitre: Enlarged thyroid gland Nodules: Abnormal growth of the thyroid gland with several causes but in most cases are an incidental finding on examination Non-toxic multinodular goitre: Thyroid goitre with multiple nodules but no hyperthyroidism Toxic multinodular goitre: Autonomous hormone-secreting nodules that result in hyperthyroidism independent of TSH feedback
Toxic multinodular goitre typically emerges from nontoxic multinodular goitres over a longer period of time. Below are two main mechanisms for the disease: 1, 2
Chronic iodine deficiency:
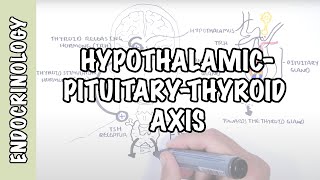
Results in decreased thyroid hormone production and consequent increased TRH secretion from the hypothalamus
Persistent TSH stimulation of the thyroid gland results in hyperplasia of thyroid tissue -> production of nodules and proliferation of existing ones
Overall leading to NON-TOXIC multinodular goitre (meaning normal thyroid hormone levels and functions overall in the body)
Long-standing multinodular goitres:
Increased risk of multiple somatic mutations of TSH receptors
Leading to a gain of function in the TSH receptors
Autonomous functioning of thyroid nodules independent of pituitary TSH feedback
Overall results in toxic multinodular goitre due to the increased release of both T3 and T4 hormones and subsequent hyperthyroidism
Thyroid releasing hormone (TRH) stimulates the release of thyroid stimulating hormone (TSH) from the pituitary gland.
TSH stimulates receptors in the thyroid gland to produce thyroid hormones T3 and T4.
Suppressed TSH: Due to autonomic functioning of thyroid nodules independent of TSH feedback
Elevated T3 and T4: Due to gain of function mutation in TSH receptor
Thyroid Ultrasound with doppler:
Determines number of thyroid nodules
Doppler done to determine vascularity (screening for thyroid cancer)
Thyroid scintigraphy: Radionuclide thyroid scan done when TSH is low
Increased “Patchy” radioiodine uptake by multiple hyperfunctioning nodules (hot areas)
Decreased uptake in surrounding thyroid tissue
Helpful in differentiating causes of hyperthyroidism
Patchy uptake on scintigraphy distinguished TMG from Graves diseases, which shows diffuse uptake, and toxic adenoma, which shows a single site of uptake.
Iodine excess triggers overproduction in autonomous tissue or latent Graves
Occurs after contrast/amiodarone exposure; underlying nodular goitre common; RAIU often low/normal due to iodine saturation; Doppler shows increased flow in type 1
Khalid N, Can AS. Plummer Disease. [Updated 2023 Mar 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK565856/
Holzapfel HP, Führer D, Wonerow P, Weinland G, Scherbaum WA, Paschke R. Identification of constitutively activating somatic thyrotropin receptor mutations in a subset of toxic multinodular goiters. J Clin Endocrinol Metab. 1997;82(12):4229-4233. doi:10.1210/jcem.82.12.4441
Hughes K, Eastman C. Thyroid disease: Long-term management of hyperthyroidism and hypothyroidism. Aust J Gen Pract. 2021;50(1–2):36–42. doi:10.31128/AJGP-09-20-5653. Available from: https://www1.racgp.org.au/ajgp/2021/january-february/thyroid-disease-long-term-management-of-hyperthyro













Discussion