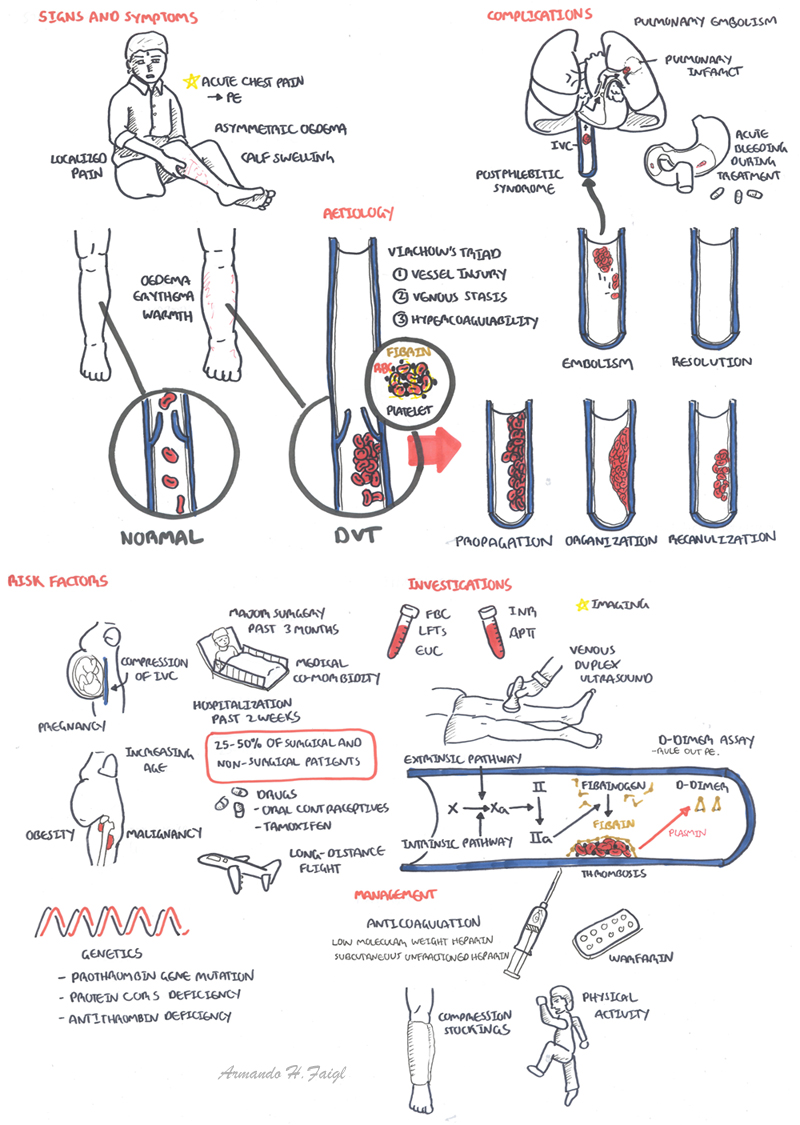
Overview Deep vein thrombosis (DVT) is the formation of a blood clot in a vein deep under the skin 25-50% of surgical patients and many non-surgical patients. 65% of DVT are below the knee are symptomatic and rarely embolism to the lung. There are many causes of DVT.
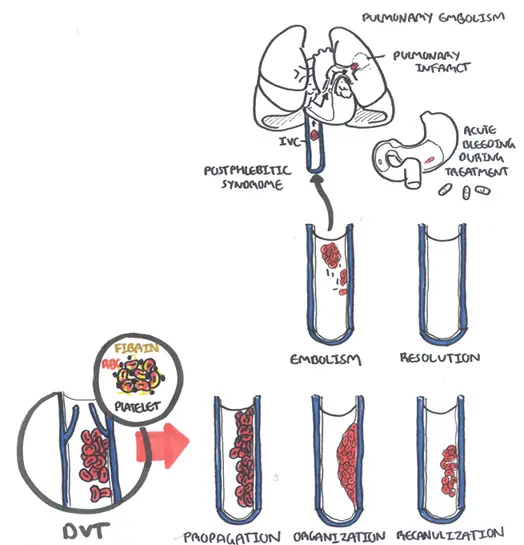
| Definition Thrombus: blood clot Thrombosis: blood clot that forms in a vessel and remains there Deep Vein Thrombosis (DVT): Formation of a blood clot in one of the deep veins of the body, usually in the leg Pulmonary Embolism (PE): occurs most often from a disloged thrombus from teh lower limb (DVT). The embolyus travels towards the lung and becomes lodged in the pulmonary artery resulting in infarction of the lung tissue. Venous Thromboembolism (VTE): Formation, development, or existence of a blood clot or thrombus within the venous system that has/potential to embolize. |
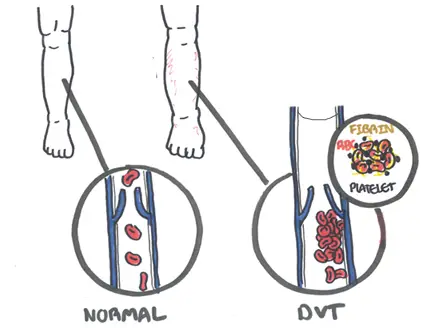
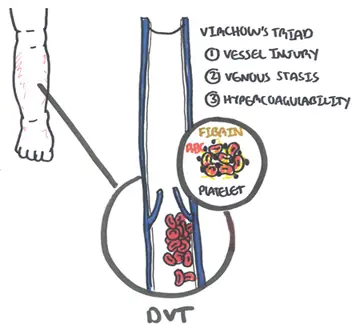
Clinical Presention DVT usually affects the veins in the legs, notably the calf.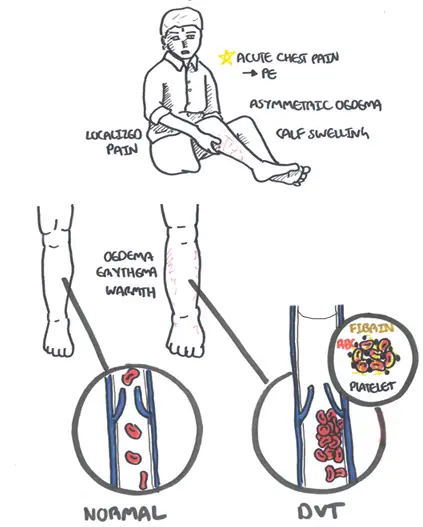
Signs of Pulmonary embolism (complication of DVT)
| MODIFIED WELL CRITERIA | |
| Clinical features | Score |
| Active cancer | 1 |
| Paralysis, paresis, or recent cast immobilization of the lower extremities | 1 |
| Recently bedridden for ≥ 3 days, or major surgery within the previous 12 weeks requiring general or regional anesthesia | 1 |
| Localized tenderness along the distribution of the deep venous system | 1 |
| Entire leg swelling | 1 |
| Calf swelling at least 3 cm larger than that on the asymptomatic side | 1 |
| Pitting edema confined to the symptomatic leg | 1 |
| Collateral superficial veins (non-varicose) | 1 |
| Previously documented deep vein thrombosis | 1 |
| Alternative diagnosis at least as likely as deep vein thrombosis | 2 |
Wells Scoring System - help tailor investigations
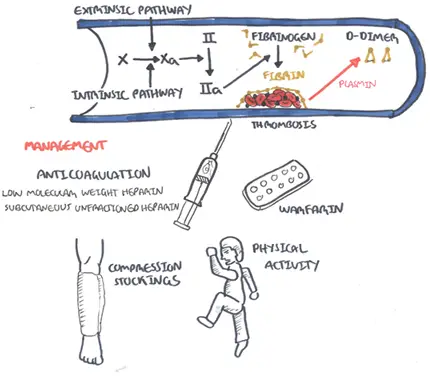
| Think D-dimer assay is only useful if it is negative; it helps in ruling out DVT |
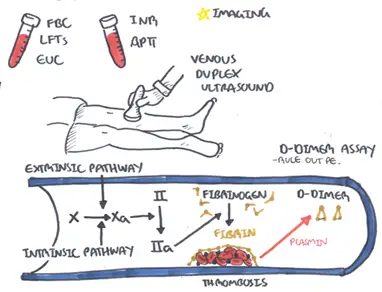
Diagnosis
All comes down to Virchow's Triad. Any change to Virchows triad increases the risk of VTE.
| Virchows Triad: Hypercoagulability, Vessel wall injury, Stasis |
Hypercoagulability
| Inherited Thombophilias |
| Factor 5 leiden mutation |
| Pro-thrombin gene mutation |
| Protein S deficiency |
| Protein C deficiency |
Stasis
Endothelial injury
The aim of treatment is to prevent PE, reduce morbidity and prevent or minimise the risk of developing the postphlebitic syndrome
| MANAGEMENT DURATION | |
| Clinical situation | Duration |
| VTE provoked by transient major risk factor | 3 months |
| Distal unprovoked DVT or PE | 3 months |
| First unprovoked proximal DVT or PE | 6 months |
First unprovoked VTE plus
|
Indefinite |
| Recurrent unprovoked VTE | Indefinite |
Complications
Prognosis
Prevention in surgery
| Remember Make sure there are no contraindications for LMWH and Mechanical prophylaxis |
| Watch Deep Vein Thrombosis |










