Liver Abscess


Author
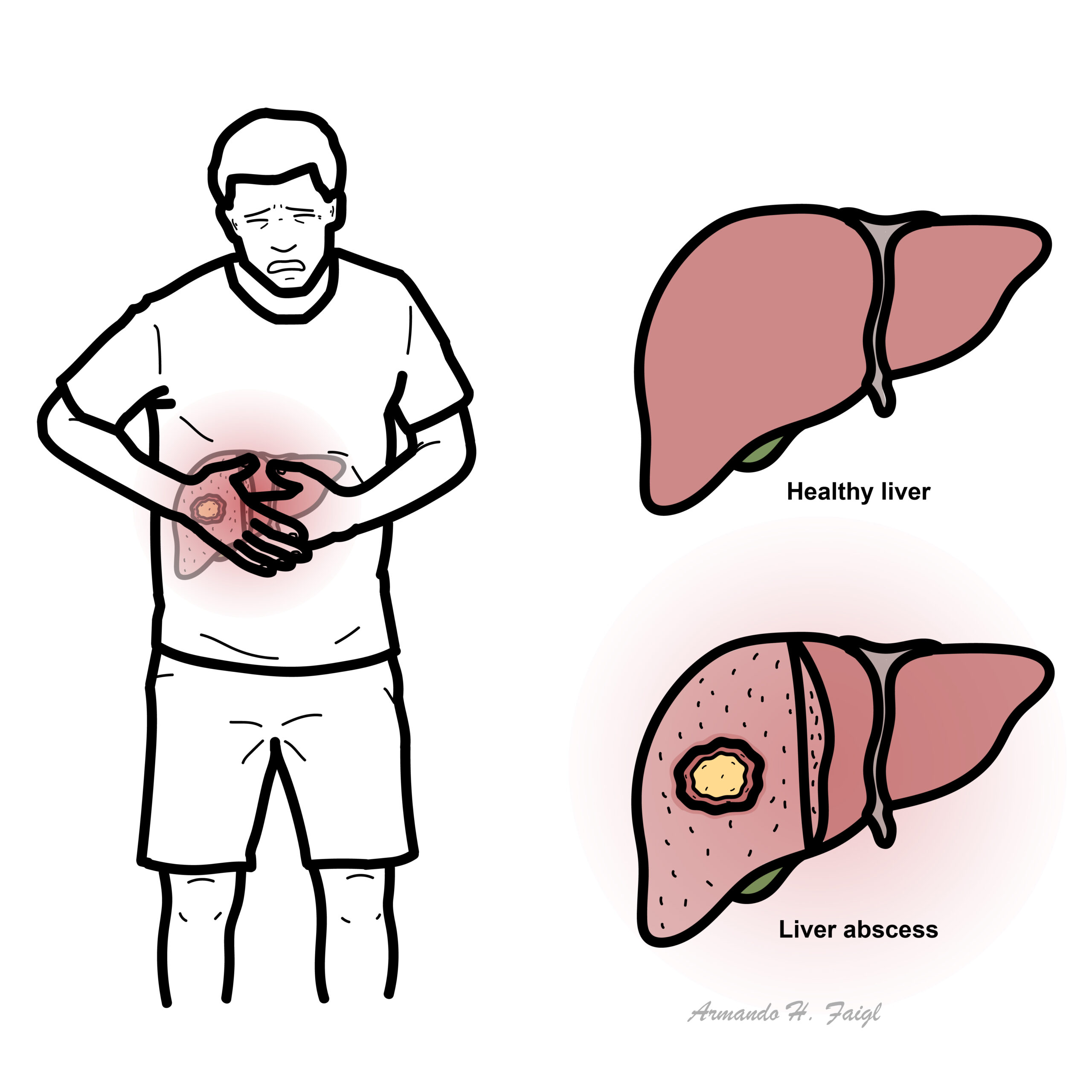
Collection of pus forming a mass in the liver as a result of infection. Mainly divided into two types
Route of infection
Since the liver receives its blood circulation from the systemic and portal circulations, it is more susceptible to getting infections and abscesses from the blood.
Can be solitary or multiple pus filled masses caused by bacteria and are generally polymicrobial involving gut-derived Gram-negative, gram positive and anaerobic organisms.
Hemochromatosis is associated with Y. enterocolitica liver abscess. Reason being the bacteria thrives in iron rich environment.
Liver abscess can be one manifestation of the highly virulent klebsiella pneumoniae. Serotypes K1 and K2 is also associated with endopthlamitis.
In patients who present with cholangitis , but who remain septic despite relief of biliary obstruction, it is vital to exclude liver abscess.
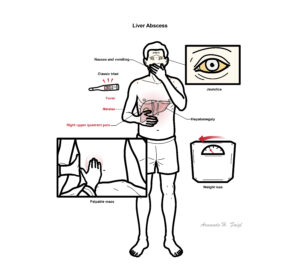
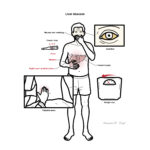
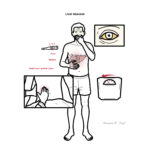
Patients complain of a classic triad of fever (with chills), right upper quadrant pain, malaise
Similar triad to ascending cholangitis – fever, RUQ pain and leukocytosis
Some may present more indolently (> 1 month) with fever of unknown origin (FUO) with non specific symptoms as nausea, vomiting and unexplained weight loss.On GPE jaundice with hepatomegaly and large mass are observed.
Examination may reveal tender hepatomegaly, and occasionally jaundice.
Elevated serum Alk phosphatase are the most common finding.
Serological test for amebiases should be done in all patients.
Secondly abdominal imaging studies are performed
The characteristic presentation is solitary or multiple lesions in the right liver lobe with a edematous surrounding parenchyma.
Abscess aspiration (if blood cultures negative and failure to respond to initial treatment).
Consider colonoscopy to exclude colon cancer in Streptococcus milleri abscess.
Percutaneous CT or Ultrasound guided drainage for lesions more than 3-5 cm.
Prolonged Antibiotics (IV and oral) 4-6 weeks
Surgical drainage
Complications include:
Prognosis for treated PLA is good but 100 percent of untreated PLAs succumb to death.
Increased morbidity is associated with increasing age, pyogenic abscess with sepsis, immunosuppression, bacteraemia, multiple comorbidities and abscesses.
Recurrence of a liver abscess is more common in patients with an underlying biliary tract abnormality than in those without biliary disease.
Infection is caused by anaerobes ,the most common being Entamoeba histolytica, which is transmitted feco-orally.
Patients usually present with fever (no chills), right upper quadrant pain, chest pain and sometimes diarrhoea. However Amebiasis presents with a variety of clinical states
The main route of infection for this protozoan is the portal vein.
E histolytica is endemic in Central and South America, Africa, and Asia thus is suspected in individuals who travel there.
The abscess is filled with a reddish brown paste like fluid and is a solitary mass in the right lobe of the liver.
Treatment
BMJ
AMBOSS
NCBI
Oxford Handbook of Gastroenterology













Discussion