

Acute Respiratory Failure

Overview
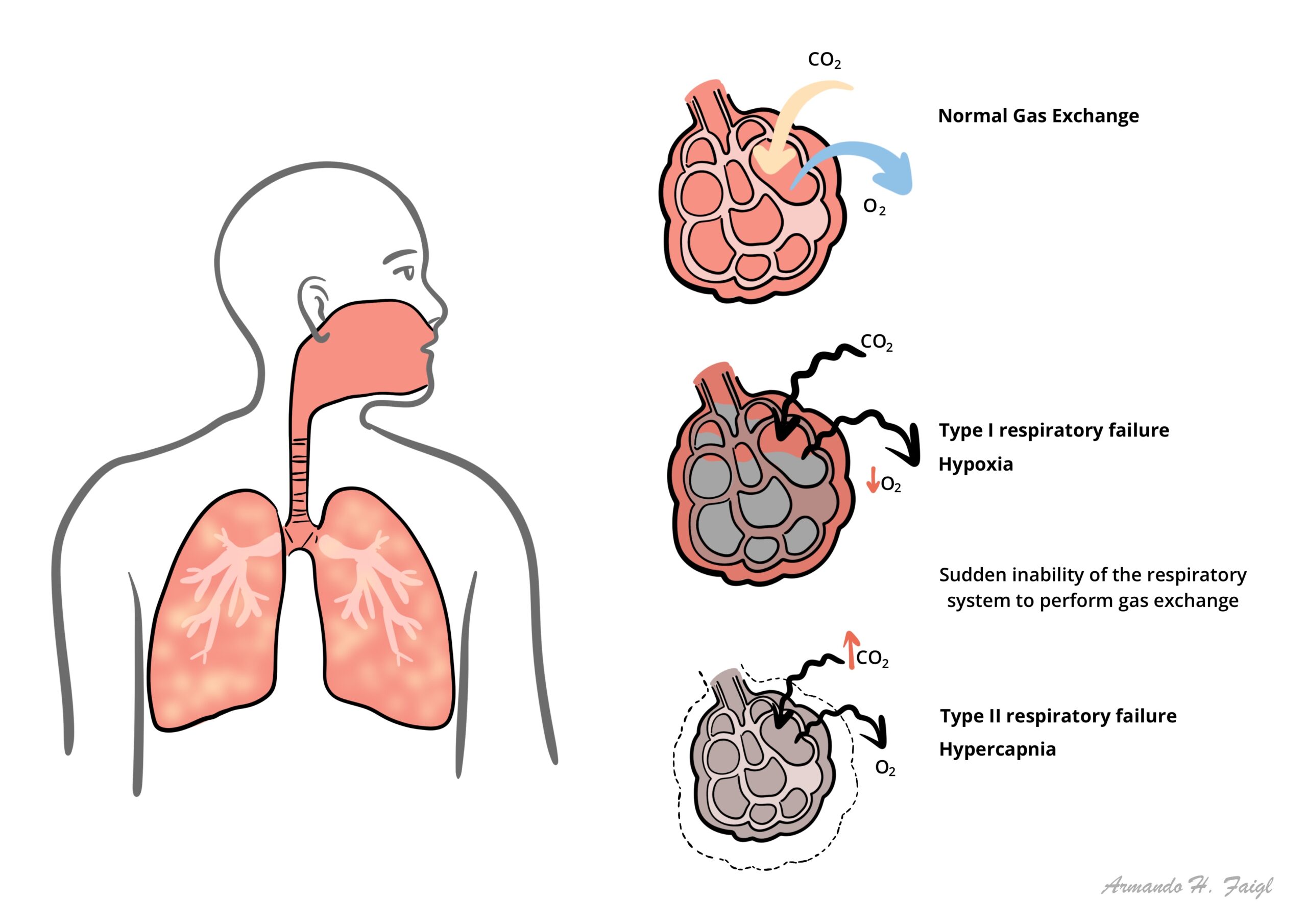
Acute Respiratory Failure (ARF) is a life-threatening impairment of the respiratory system’s ability to maintain adequate gas exchange. It occurs when the lungs fail to adequately oxygenate systemic arterial blood, fail to eliminate carbon dioxide produced by tissue metabolism, or both. ARF is not a disease entity in itself, but rather a sudden, critical physiological breakdown resulting from a wide spectrum of pulmonary, cardiac, neuromuscular, or central nervous system disorders.
Rapid recognition and classification are vital because unmanaged respiratory failure rapidly culminates in tissue hypoxia, multi-organ failure, cardiac arrest, and death. Management requires immediate stabilization of the airway and oxygenation, determination of whether the failure is hypoxemic (Type 1) or hypercapnic (Type 2), and targeted treatment of the underlying cause alongside supportive mechanical ventilation when indicated.
Definition
Hypoxemic Respiratory Failure (Type 1): Inability to adequately oxygenate arterial blood, defined as a PaO2 < 60 mmHg (8.0 kPa) on room air.
Hypercapnic Respiratory Failure (Type 2): Inability to adequately eliminate carbon dioxide, defined as a PaCO2 > 45 mmHg (6.0 kPa) with an arterial pH < 7.35.
Alveolar-Arterial (A-a) Gradient: The difference between alveolar oxygen concentration (PAO2) and arterial oxygen concentration (PaO2); helps differentiate intrinsic pulmonary pathology from pure hypoventilation or low inspired oxygen.
Intrapulmonary Shunt: Perfusion of unventilated alveoli (V/Q = 0) leading to deoxygenated blood entering systemic circulation; hypoxemia from a true shunt is refractory to supplemental oxygen.
Atelectasis: Collapse or closure of lung alveoli resulting in reduced functional residual capacity and V/Q mismatch.
Classification
Type 1 – Hypoxemic Respiratory Failure
- Definition: PaO2 < 60 mmHg with a normal or low PaCO2.
- Pathology: Primary defect is impaired oxygen transfer across the alveolar-capillary membrane.
- A-a Gradient: Characterized by an elevated A-a gradient.
Type 2 – Hypercapnic Respiratory Failure
- Definition: PaCO2 > 45 mmHg accompanied by acute respiratory acidosis (pH < 7.35).
- Pathology: Primary defect is alveolar hypoventilation (failure of minute ventilation).
- A-a Gradient: Characterized by a normal A-a gradient if lungs are structurally normal, or an elevated A-a gradient if co-existing parenchymal disease is present.
Type 3 – Perioperative Respiratory Failure
- Subtype: Caused by post-operative atelectasis, reduced functional residual capacity, and shallow breathing secondary to abdominal/thoracic pain or anesthesia.
Type 4 – Shock-Related Respiratory Failure
Subtype: Secondary to systemic hypoperfusion where respiratory muscles receive inadequate cardiac output, leading to respiratory muscle fatigue.
Type 1 is oxygenation failure (PaO2 < 60 mmHg with normal/low PaCO2), while Type 2 is ventilation failure (PaCO2 > 45 mmHg with acidosis pH < 7.35).
Aetiology & Risk Factors
Type 1 (Hypoxemic) Causes
- V/Q Mismatch: Pneumonia, Pulmonary Edema, Chronic Obstructive Pulmonary Disease (COPD), Asthma, Atelectasis.
- Intrapulmonary Shunt: Acute Respiratory Distress Syndrome (ARDS), severe lobar pneumonia, pulmonary alveolar proteinosis.
- Diffusion Limitation: Idiopathic Pulmonary Fibrosis, interstitial lung disease, systemic sclerosis.
- Vascular Disruption: Pulmonary Embolism (PE), pulmonary arterial hypertension.
Type 2 (Hypercapnic) Causes
- Central Nervous System Depression: Opioid/sedative overdose, brainstem stroke, traumatic brain injury, central sleep apnea.
- Neuromuscular Disorders: Guillain-Barré Syndrome, Myasthenia Gravis, Amyotrophic Lateral Sclerosis (ALS), cervical spinal cord injury.
- Chest Wall & Pleural Defects: Flail chest, severe kyphoscoliosis, obesity hypoventilation syndrome, massive pleural effusion.
- Severe Airway Obstruction: End-stage COPD, severe acute asthma, upper airway obstruction (foreign body, anaphylaxis, vocal cord paralysis).
Hypoxemia with a normal A-a gradient is caused by either alveolar hypoventilation (e.g., opioid overdose) or low FiO2 (e.g., high altitude). Hypoxemia with an elevated A-a gradient indicates intrinsic lung disease (V/Q mismatch, shunt, or diffusion defect).
Pathophysiology
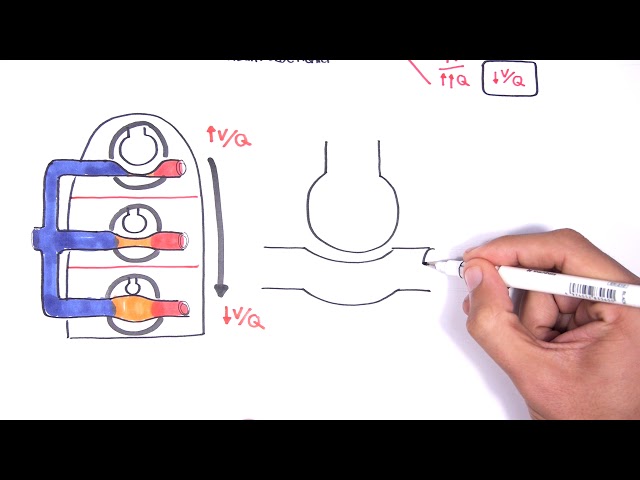
- V/Q Mismatch: Regions of lung receive ventilation without adequate perfusion (dead space, V/Q > 1) or perfusion without adequate ventilation (shunt, V/Q < 1).
- Intrapulmonary Shunting: Blood passes through non-ventilated alveoli; supplemental oxygen cannot raise PaO2 significantly because oxygen cannot reach the blood passing through collapsed alveoli.
- Alveolar Hypoventilation: Reduced minute ventilation (Tidal Volume x Respiratory Rate) leads directly to CO2 accumulation according to the alveolar ventilation equation.
- Diffusion Impairment: Thickening or destruction of the alveolar-capillary membrane impairs oxygen transport (exacerbated during exercise or high cardiac output states).
Shunt physiology (V/Q = 0) is refractory to supplemental oxygen therapy because the inspired oxygen never reaches the blood flowing past non-ventilated alveoli.
Clinical Manifestations
Hypoxemia Manifestations
- Severe dyspnoea, tachypnoea
- Central cyanosis
- Nasal flaring
- Intercostal retractions.
- Tachycardia, arrhythmias
- Hypotension, and bradycardia (late sign preceding cardiac arrest).
- Agitation, anxiety, confusion, delirium
- Decreased level of consciousness.
Hypercapnia Manifestations
- Morning headache (due to nocturnal cerebral vasodilation), somnolence
- Confusion
- Asterixis (flapping tremor)
- Obtundation
- Papilledema.
- Warm, flushed peripheries
- Diaphoresis, bounding pulses
Signs of Respiratory Muscle Fatigue & Impending Collapse
- Tachypnoea (> 35 breaths/min): Initial attempt to compensate for reduced tidal volume or hypoxemia.
- Paradoxical Abdominal Breathing: Abdomen moves inward during inspiration due to diaphragmatic exhaustion.
- Tachypnoea to Bradypnoea Shift: A sudden drop in respiratory rate in a struggling patient indicates impending respiratory arrest.
A patient with acute respiratory failure who shifts from tachypnea to bradypnea is experiencing diaphragmatic exhaustion and requires immediate endotracheal intubation.
Diagnosis
Arterial Blood Gas (ABG – Gold Standard)
- PaO2 < 60 mmHg: Confirms hypoxemia (Type 1).
- PaCO2 > 45 mmHg with pH < 7.35: Confirms acute hypercapnic respiratory failure (Type 2).
- Serum Bicarbonate (HCO3-): Normal in acute respiratory acidosis (uncompensated); elevated in chronic respiratory acidosis (renal compensation).
Calculated Indices
- A-a Gradient: PAO2 – PaO2. Normal is < 10–15 mmHg (or [Age / 4] + 4).
- PaO2 / FiO2 Ratio: Used to assess severity in acute lung injury / ARDS.
Imaging
- Chest X-Ray
- Identifies parenchymal lung disease (pneumonia, edema, atelectasis, pneumothorax, effusion).
- CT Pulmonary Angiogram (CTPA)
- Gold standard for suspected Pulmonary Embolism.
- High-Resolution CT (HRCT)
- Evaluates interstitial lung disease.
Bedside & Neuromuscular Assessment
- Negative Inspiratory Force (NIF) / Maximum Inspiratory Pressure (MIP): NIF less negative than -20 cmH2O indicates severe respiratory muscle weakness.
- Forced Vital Capacity (FVC): FVC < 15–20 mL/kg indicates impending neuromuscular respiratory failure (e.g., in Guillain-Barré).
- Peak Expiratory Flow Rate (PEFR): Evaluates severe airflow obstruction in asthma/COPD.
In neuromuscular diseases (e.g., Guillain-Barré, Myasthenia Gravis), monitor FVC (< 20 mL/kg) and NIF (less negative than -20 cmH2O) to identify the need for elective intubation BEFORE ABG abnormalities develop.
Treatment
Immediate Airway & Oxygenation Management
- Target Oxygen Saturation:
- Type 1 Failure: Target SpO2 >= 94–98%.
- Type 2 Failure (COPD / Hypercapnic Risk): Target SpO2 88–92% to prevent loss of hypoxic drive and worsening V/Q mismatch.
- Oxygen Delivery Devices: Nasal cannula, Venturi mask (precise FiO2 delivery for COPD), or High-Flow Nasal Cannula (HFNC).
Non-Invasive Ventilation (NIV)
- Continuous Positive Airway Pressure (CPAP): Recruits collapsed alveoli; first-line for cardiogenic pulmonary edema and atelectasis.
- Bilevel Positive Airway Pressure (BiPAP): Provides IPAP (supports ventilation/CO2 removal) and EPAP (maintains airway patency); first-line for acute hypercapnic exacerbation of COPD.
Invasive Mechanical Ventilation (Intubation)
- Indications: Severe hemodynamic instability, altered mental state/inability to protect airway, failed NIV trial, severe acidosis (pH < 7.20), or respiratory arrest.
Targeted Etiological Therapy
- Bronchodilators & Systemic Corticosteroids for asthma and COPD exacerbations.
- Antibiotics / Antivirals for pneumonia or infectious bronchitis.
- IV Diuretics for cardiogenic pulmonary edema.
- Reversal Agents
- Naloxone for opioid toxicity
- Flumazenil for benzodiazepine overdose (use with caution due to seizure risk).
- Anticoagulation for Pulmonary Embolism.
BiPAP is the non-invasive ventilation of choice for Type 2 hypercapnic failure (COPD exacerbations), whereas CPAP is first-line for Type 1 hypoxemic failure (cardiogenic pulmonary edema).
Complications & Prognosis
- Cardiac arrhythmias
- Acute cor pulmonale
- Cardiac arrest
- Ventilator-Induced Lung Injury (VILI – barotrauma, volutrauma)
- Ventilator-Associated Pneumonia (VAP)
- Pulmonary fibrosis.
- Hypoxic-ischemic encephalopathy
- Stress-induced gastrointestinal ulceration/bleeding
- Deep Vein Thrombosis (DVT) / PE
- Acute Kidney Injury
- In-hospital mortality varies from 10–30% for COPD-related hypercapnic failure up to 40–50% for ARDS and severe sepsis-induced Type 1 failure.
- Predictors of Poor Outcome: Advanced age, multi-organ dysfunction, delayed intubation, severe underlying chronic organ disease, and low baseline functional status.
References
- Roussos C, Koutsoukou A. Respiratory failure. Eur Respir J Suppl. 2003;47:3s-14s. doi:10.1183/09031936.03.00038503
- Vincent JL, Hall JB. Acute respiratory failure. N Engl J Med. 2012;367(25):2451-2452. doi:10.1056/NEJMc1212879
- Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50(2):1602426. doi:10.1183/13993003.02426-2016





Members only discussions coming soon…