

Systemic Sclerosis (SSc)
Overview
Systemic sclerosis (SSc), also known as scleroderma, is a rare chronic autoimmune connective tissue disease characterized by fibrosis, vasculopathy, and autoimmunity. It primarily affects the skin but can also involve the lungs, GI tract, kidneys, and heart. The estimated prevalence is 50–300 per million, with a female-to-male ratio of ~4:1, and peak onset between 30–50 years. There are two main clinical subsets: limited cutaneous (lcSSc) and diffuse cutaneous (dcSSc), with differing organ involvement and prognosis.
Definition
Systemic sclerosis (SSc): Chronic autoimmune disease with progressive fibrosis of skin and internal organs, vasculopathy, and specific autoantibodies.
CREST syndrome: Subset of limited SSc (Calcinosis, Raynaud’s, Esophageal dysmotility, Sclerodactyly, Telangiectasia).
Fibrosis: Excess deposition of extracellular matrix (mainly collagen).
Raynaud’s phenomenon: Episodic vasospasm of digits in response to cold/stress.
Aetiology & Risk Factors
- Unknown precise trigger
- Likely combination of genetic predisposition, immune dysregulation, and environmental exposures
- Genetic: HLA-DRB1, HLA-DQB1 associations
- Female predominance
- Occupational: Silica, solvents (e.g. vinyl chloride), epoxy resins
- Infection: Possible viral triggers (e.g. CMV, parvovirus B19)
Pathophysiology
- Endothelial injury → immune cell recruitment and endothelial apoptosis
- Vascular dysfunction → intimal proliferation, luminal narrowing, and obliteration
- Immune activation → release of pro-fibrotic cytokines (TGF-β, IL-6)
- Fibroblast activation → excessive extracellular matrix and collagen deposition
- Progressive tissue fibrosis → skin thickening and organ dysfunction
TGF-β is the central cytokine driving fibrosis.
Clinical Manifestations
| Feature | Limited Cutaneous SSc (lcSSc) | Diffuse Cutaneous SSc (dcSSc) |
| Skin Involvement | Distal to elbows and knees (face, hands, forearms, feet) | Proximal and distal limbs, trunk, face |
| Onset & Progression | Gradual onset; slow progression | Rapid onset; early organ involvement |
| Raynaud’s Phenomenon | Precedes skin changes by months/years | Occurs concurrently or after skin changes |
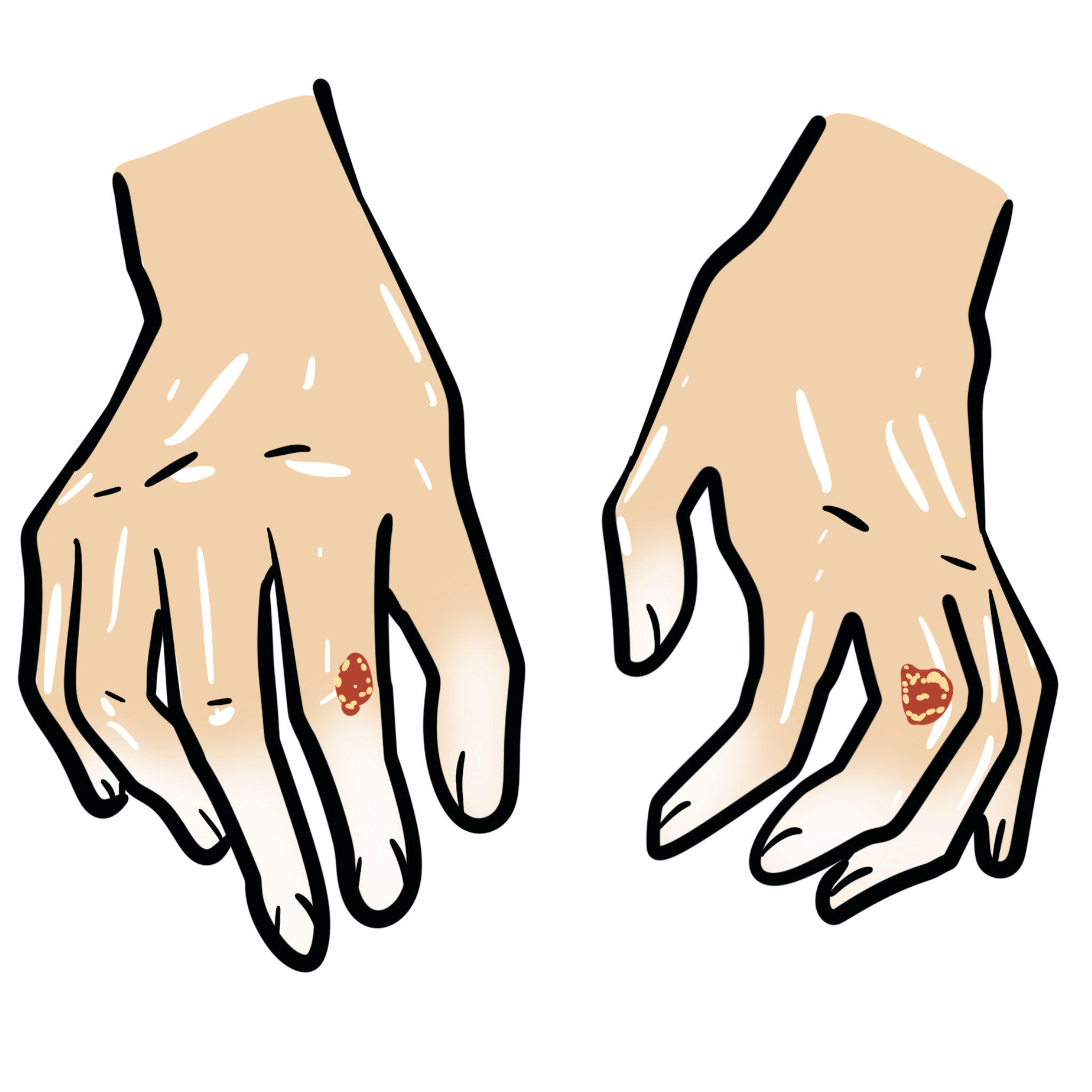
| Skin Features | Sclerodactyly, digital ulcers, telangiectasias, calcinosis cutis (CREST) | Sclerodactyly, diffuse skin thickening, hyperpigmentation |
| GI Involvement | Esophageal dysmotility common; late small bowel involvement | Early and more severe GI involvement (including malabsorption, pseudo-obstruction) |
| Pulmonary Involvement | Pulmonary arterial hypertension (PAH) more common | Interstitial lung disease (ILD) more common |
| Renal Involvement | Rare | Scleroderma renal crisis (SRC) — life-threatening |
| Cardiac Involvement | Arrhythmias possible | More common: myocarditis, pericardial effusion, conduction defects |
| Vascular Manifestations | Telangiectasia, digital ischemia | Digital ischemia, fingertip pitting/scars |
| Autoantibodies | Anti-centromere (ACA) | Anti-Scl-70 (topoisomerase I), anti-RNA polymerase III |
Raynaud’s may predate systemic symptoms by years — always screen ANA and ENA in persistent cases.
CREST
Calcinosis cutis
Raynaud’s phenomenon
Esophageal dysmotility
Sclerodactyly
Telangiectasia
Diagnosis
Diagnostic Criteria: 2013 ACR/EULAR Criteria
- Score ≥9 = classification as SSc
- Skin thickening of fingers of both hands extending proximal to MCPs = automatic diagnosis
- Other weighted criteria:
– Puffy fingers, fingertip ulcers/scars, telangiectasia
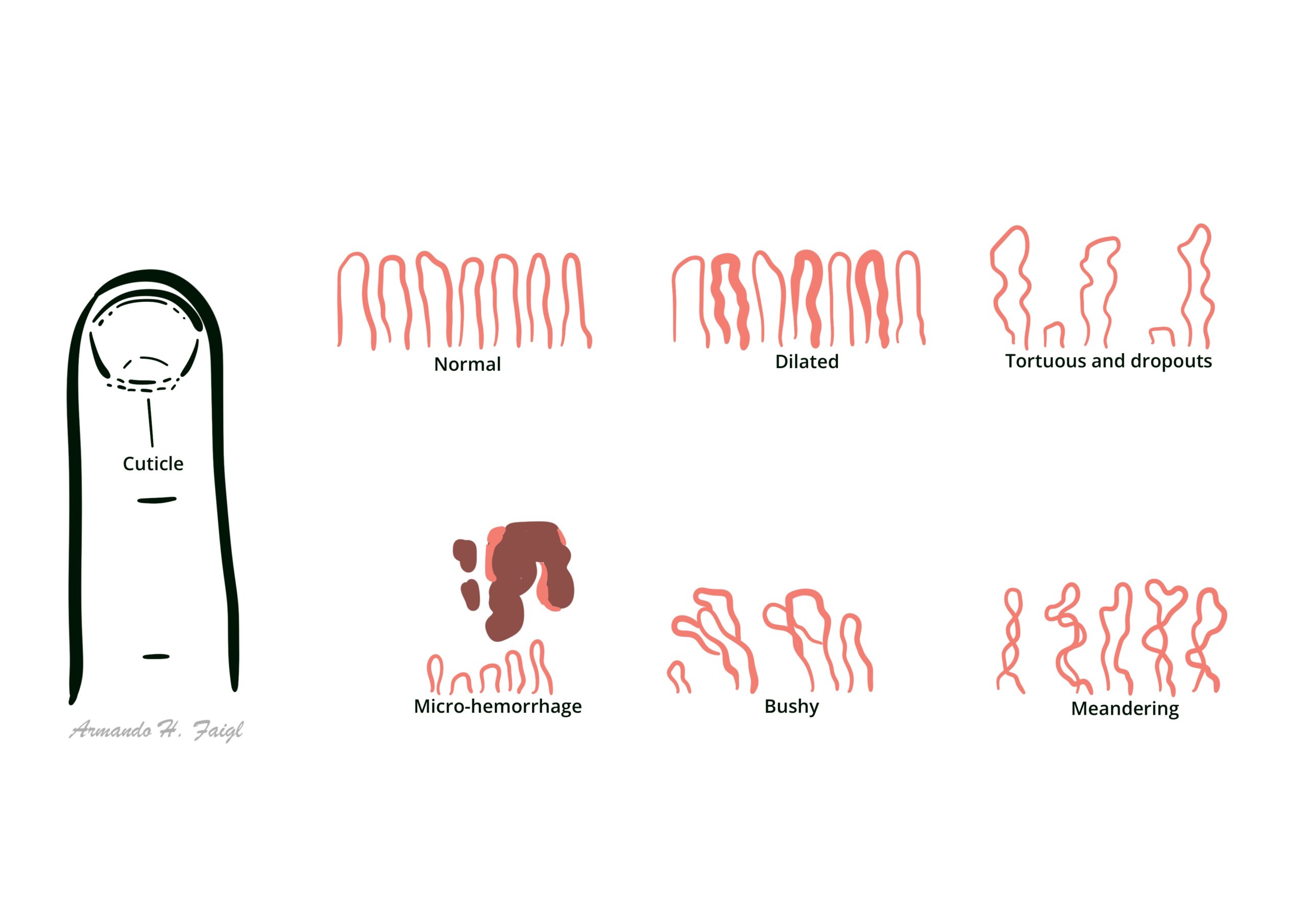
– Nailfold capillary abnormalities
– Pulmonary hypertension or ILD
– Raynaud’s phenomenon
– SSc-specific autoantibodies (anti-centromere, anti-Scl-70, anti-RNA pol III)
- ANA: positive in >90%
- Specific antibodies
- Anti-centromere (lcSSc)
- Anti-Scl-70 / anti-topoisomerase I (dcSSc, ILD)
- Anti-RNA polymerase III (renal crisis, dcSSc)
- Nailfold capillaroscopy: abnormal dilated capillaries
- HRCT chest: ILD, ground-glass opacities
- Echocardiogram + NT-proBNP: screen for PAH
- Barium swallow/manometry: assess esophageal dysmotility
- Creatinine, urinalysis: monitor for renal crisis
RNA polymerase III is associated with rapid scleroderma, renal criss and GAVE.
Differential Diagnoses
| Condition | Differentiating Feature |
| SLE | Malar rash, arthritis, more systemic but no skin thickening |
| Dermatomyositis | Heliotrope rash, proximal muscle weakness, Gottron’s papules |
| Mixed CTD | Overlapping features; high anti-U1 RNP |
| Eosinophilic fasciitis | Skin tightening sparing fingers, eosinophilia |
| Scleromyxedema | Generalized waxy papules, mucin deposition, monoclonal gammopathy (usually IgG λ), no Raynaud’s, no internal organ fibrosis |
Use nailfold capillaroscopy + ENA panel in all cases with Raynaud’s + skin symptoms.
Classification
| Subtype | Features |
| Limited cutaneous (lcSSc) | Distal skin involvement (fingers, face), CREST, late organ involvement, anti-centromere antibodies |
| Diffuse cutaneous (dcSSc) | Proximal limb/trunk skin thickening, early organ fibrosis, renal crisis, anti-Scl-70/RNA pol III |
| Sine scleroderma | Internal organ involvement without skin changes |
| Overlap syndromes | Features of SSc + another CTD (e.g. SLE, myositis) |
Treatment
No cure — aim to control symptoms and prevent complications
- Raynaud’s
- Calcium channel blockers (nifedipine), sildenafil, topical nitrates
- Avoid cold, smoking; hand warmers
- Skin fibrosis
- Methotrexate or mycophenolate (off-label use)
- Rituximab (for refractory cases)
- Tocilizumab
- Lung involvement
- Mycophenolate mofetil (ILD)
- Cyclophosphamide (alternative)
- Nintedanib (anti-fibrotic approved for SSc-ILD)
- Autologous stem cell transplant (ASCT)
- Pulmonary hypertension
- Endothelin receptor antagonists (bosentan)
- PDE-5 inhibitors (sildenafil)
- Prostacyclin analogs
- Scleroderma renal crisis:
- ACE inhibitors (e.g. captopril) — initiated early and continued long-term
- Dialysis
- GI management
- PPI for reflux
- Prokinetics (metoclopramide) for dysmotility
- Antibiotics for SIBO
Supportive
• Annual echocardiogram (or pBNP) and PFTs
• Occupational therapy for hand function
• Regular BP monitoring
ACE inhibitors are life-saving in scleroderma renal crisis.
ASCT should only be considered in high-volume centers with multidisciplinary teams. Careful pre-transplant cardiac screening is essential due to risk of treatment-related mortality. HSCT does not cure systemic sclerosis but may induce long-term remission in selected patients.
Complications & Prognosis
Complications
- ILD and PAH (leading causes of death)
- Renal crisis
- GI malabsorption, GAVE
- Skin ulcers, infections
Poor Prognostic Factors
- Diffuse cutaneous subtype
- Male gender
- African ancestry
- Early organ involvement: PAH/ILD
- Anti-RNA polymerase III positivity
- Elevated CRP, anemia
In young patients with early aggressive dcSSc and deteriorating lung function despite immunosuppression, refer early for HSCT evaluation.
References
- van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2013;65(11):2737–2747.
- Denton CP, Khanna D. Systemic sclerosis. Lancet. 2017;390(10103):1685–1699.
- Distler O, Highland KB, Gahlemann M, et al. Nintedanib for systemic sclerosis-associated interstitial lung disease. N Engl J Med. 2019;380(26):2518–2528.
- Tashkin DP, Elashoff R, Clements PJ, et al. Cyclophosphamide vs placebo in scleroderma lung disease. N Engl J Med. 2006;354(25):2655–2666.
- Allanore Y, Simms R, Distler O, et al. Systemic sclerosis. Nat Rev Dis Primers. 2015;1:15002.








Members only discussions coming soon…