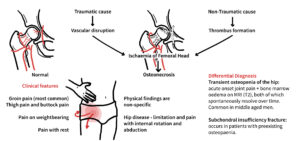
Osteonecrosis of the hip, usually referring to osteonecrosis of the femoral head (ONFH), is a progressive disorder caused by compromised subchondral blood supply leading to death of osteocytes and marrow elements, failed structural repair, subchondral fracture, femoral head collapse, and eventually secondary hip osteoarthritis.[1-4]
It most often affects younger to middle-aged adults, commonly between 20 and 50 years, and is an important cause of hip disability in otherwise active patients.[2-4]
Reported epidemiology varies by region; commonly cited estimates include about 10,000–20,000 new cases annually in the United States, and atraumatic disease may be bilateral in a substantial proportion of patients.[1,3,4]
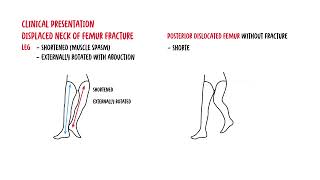
Major associated exposures are corticosteroids and alcohol, while traumatic cases follow femoral neck fracture or hip dislocation.[1-4]
Think of ONFH in a young or middle-aged adult with groin pain plus steroid exposure, alcohol excess, sickle cell disease, lupus, transplant history, or prior hip trauma.
Early diagnosis matters because precollapse disease may still be amenable to joint-preserving treatment.
Definition
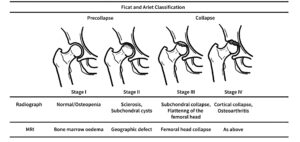
Osteonecrosis: death of bone and marrow cellular elements due to impaired blood supply; in the hip this usually involves the subchondral femoral head. Femoral head collapse: structural failure of the necrotic subchondral bone, often following subchondral fracture, causing loss of sphericity. Crescent sign: subchondral radiolucent line on radiographs indicating subchondral fracture and impending or established collapse. Double-line sign:MRI feature on T2-weighted imaging with inner bright and outer dark rim at the interface of necrotic and reparative bone; highly suggestive of ONFH. Core decompression: hip-preserving surgical procedure that reduces intraosseous pressure and aims to improve perfusion in early-stage disease.
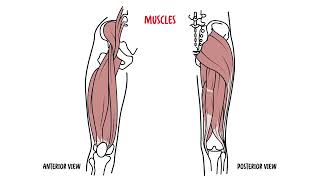
Anatomy and Physiology
The femoral head is supplied mainly by retinacular branches arising from the medial femoral circumflex artery; contribution from the artery of the ligamentum teres is limited in adults.
The subchondral region of the femoral head is especially vulnerable because it is highly load-bearing and has relatively limited collateral circulation.
Normal hip function depends on a spherical femoral head, intact subchondral plate, healthy articular cartilage, and congruent load transfer across the acetabulum
Even before cartilage damage occurs, failure of the underlying subchondral bone can distort the articular surface and drive secondary osteoarthritis.
Atraumatic disease is often bilateral, so once one hip is diagnosed the other hip warrants scrutiny, often with MRI if suspicion is high.
Steroids and alcohol are the two classic non-traumatic associations.
Absence of a clear risk factor does not exclude ONFH; idiopathic cases occur. Idiopathic ONFH is common, infact bilateral involvement is also common make sure to check the other hip!
Risk factors often converge on a final common pathway: marrow fat hypertrophy, venous stasis, thrombosis, ischemia, and impaired bone repair.
Pathophysiology
Initial vascular compromise occurs through arterial interruption, venous stasis, intramedullary hypertension, thrombosis, fat-cell hypertrophy, or microembolic phenomena depending on the cause.
Ischemia causes death of osteocytes and marrow cells within the necrotic segment.
A reparative interface develops between viable and necrotic bone, but creeping substitution is mechanically insufficient in the loaded subchondral region.
Repetitive weight-bearing leads to microfractures in weakened subchondral bone.
Subchondral fracture develops, often seen radiographically as the crescent sign or on CT/MRI before plain film change is obvious.
Once the articular surface loses support, femoral head flattening/collapse follows.
Progressive incongruity leads to cartilage degeneration, acetabular change, and secondary osteoarthritis.
This image series is only available to members
The size and location of the necrotic lesion, especially superolateral weight-bearing involvement, are major predictors of collapse.
Patients may feel relatively little early on, but the biomechanics may already be worsening; imaging stage and lesion size matter more than symptoms alone for prognosis.
Clinical Manifestations
Gradual onset deep groin pain is classic; pain may also localize to the buttock, lateral hip, anterior thigh, or be referred to the knee.
Early disease may be asymptomatic, especially when incidentally detected on MRI.
Pain is usually worse with weight-bearing and activity, then progresses to pain at rest and night pain with advancing collapse.
Limp or antalgic gait may develop as disease progresses.
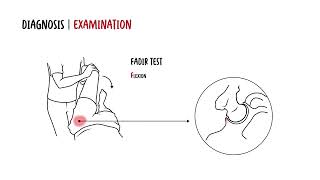
Restricted internal rotation is a key early examination clue
flexion and abduction may later become limited.
Pain is often reproduced at end-range internal rotation (but this is not specific as this happens in OA)
Advanced disease may show claudication-like gait, reduced range of motion, muscle wasting, and signs of secondary osteoarthritis.
This image series is only available to members
Diagnosis
Diagnostic criteria
Practical diagnosis is based on compatible clinical featuresplus characteristic MRI findings
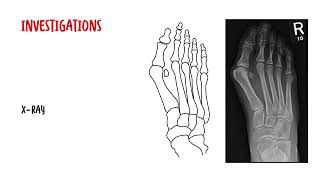
Plain radiographs (AP pelvis + frog-leg lateral): first-line, may be normal in early disease; later show sclerosis, cystic change, crescent sign, flattening, and secondary OA.[1,5]
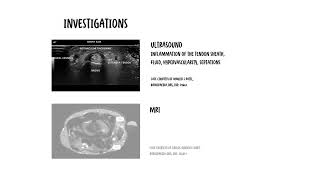
MRI: best test for early disease; highly accurate, with meta-analytic sensitivity around 91–93% and specificity around 91–96% for early ONFH.
CT: useful for detecting subchondral fracture/collapse and defining bony architecture when radiographs are equivocal.
Bone scan/SPECT: less specific than MRI; can help detect multifocal disease in selected settings.
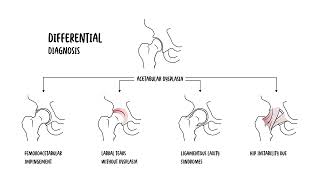
Differential diagnoses
Differential
Helpful differentiating features
Transient osteoporosis / bone marrow edema syndrome of the hip
Sudden painful syndrome, often self-limited over months; MRI marrow edema is diffuse and may extend into neck/trochanter, without the typical band-like low-signal interface of ONFH.[1,9]
Subchondral insufficiency fracture of the femoral head
More often older osteoporotic patients, acute pain, inability to walk; MRI shows subchondral low-signal fracture line with surrounding edema, and may mimic ONFH.[1,10]
Hip osteoarthritis
Joint-space loss and osteophytes predominate; ONFH classically shows focal subchondral necrosis/collapse pattern.[1,3]
Acetabular dysplasia with secondary OA
Undercoverage of femoral head, dysplastic morphology, secondary degenerative change.[1]
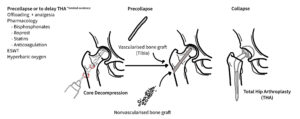
Bisphosphonates, anticoagulants, vasodilators, statins, and biophysical treatments have been explored, but evidence remains mixed and not definitive for routine standard use.
Hip-preserving surgery
Core decompression: most commonly used in early/precollapse disease; best suited before substantial collapse.
Core decompression + biologic augmentation (e.g., bone marrow aspirate concentrate): promising in some studies, but overall benefit remains controversial and inconsistent, particularly for larger lesions.
Nonvascularized bone grafting / structural grafting: considered in selected precollapse or limited-collapse lesions.
Vascularized bone grafting: aims to restore structural support and blood supply; may be considered in younger patients with limited collapse.
Osteotomy: shifts the necrotic segment away from the weight-bearing dome; used selectively in specialist centers.
Arthroplasty
Total hip arthroplasty (THA): standard option for advanced collapse, secondary OA, severe pain, or failed joint-preserving treatment.
This image series is only available to members
Precollapse disease = try to preserve the femoral head. Postcollapse with secondary OA = THA becomes the dominant option.
Chronic pain, gait impairment, and reduced function
Bilateral hip involvement
Need for THA, often at a younger age than typical degenerative OA patients
Prognosis
Small precollapse lesions may remain stable, but many untreated lesions progress.
Once collapse occurs, joint preservation is less predictable and prognosis worsens substantially.
Untreated AVN commonly progresses to secondary arthritis; one review cites progression to secondary hip arthritis in roughly 70–80% if untreated.
References
Zhao D, Zhang F, Wang B, Liu B, Li L, Kim SY, et al. Guidelines for clinical diagnosis and treatment of osteonecrosis of the femoral head in adults (2019 version). J Orthop Translat. 2020;21:100-10.
Choi HR, Steinberg ME, Cheng EY. Osteonecrosis of the femoral head: diagnosis and classification systems. Curr Rev Musculoskelet Med. 2015;8(3):210-20.
Konarski W, Poboży T, Śliwczyński A, Kotela I, Krakowiak J, Hordowicz M, et al. Avascular necrosis of femoral head—overview and current state of the art. Int J Environ Res Public Health. 2022;19(12):7348.
Hines JT, Jo WL, Cui Q, Mont MA, Koo KH, Cheng EY, et al. Osteonecrosis of the femoral head: an updated review of ARCO on pathogenesis, staging and treatment. J Korean Med Sci. 2021;36(24):e177.
American College of Radiology. ACR Appropriateness Criteria® Osteonecrosis [Internet]. Reston (VA): American College of Radiology; updated 2022 [cited 2026 Apr 20].
Yoon BH, Mont MA, Koo KH, Chen CH, Cheng EY, Cui Q, et al. The 2019 revised version of Association Research Circulation Osseous staging system of osteonecrosis of the femoral head. J Arthroplasty. 2020;35(4):933-40.
Zhang YZ, Cao XY, Li XC, et al. Accuracy of MRI diagnosis of early osteonecrosis of the femoral head: a meta-analysis and systematic review. J Orthop Surg Res. 2018;13(1):167.
Ko YS, Lee YK, Ha YC, Koo KH. Updating osteonecrosis of the femoral head. Hip Pelvis. 2023;35(3):147-55.
Maisi N, Apergis A, Kelekis A. Transient hip osteoporosis: etiopathogenetic, clinical, and imaging approach. J Clin Med. 2022;11(19):5807.
Gaudiani MA, White PB, Deren ME, et al. Subchondral insufficiency fractures of the femoral head. J Hip Preserv Surg. 2020;7(1):85-97.
Jawad MU, Haleem AA, Scully SP. In brief: Ficat classification: avascular necrosis of the femoral head. Clin Orthop Relat Res. 2012;470(9):2636-9.
Salman LA, Whyte MB, Ali AM, et al. The outcomes of total hip replacement in osteonecrosis versus osteoarthritis: a systematic review and meta-analysis. Hip Int. 2023;33(6):679-89.
Matthews AH, Davis DD, Fish MJ. Avascular necrosis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.













Discussion