
| Cardinal features of intestinal obstruction: vomiting, colicky pain, constipation and distension |
- Cardinal features of bowel obstruction present?
- Degree of obstruction to flow (partial or complete)
- Site of obstruction (small bowel or large bowel)
- Mechanical obstruction or ileus?
- Absence or presence of intestinal ischemia (simple or strangulated).
Cardinal features of bowel obstruction?
- Colicky abdominal pain
- Distension
- Absolute constipation/obstipation
- Nausea and Vomiting
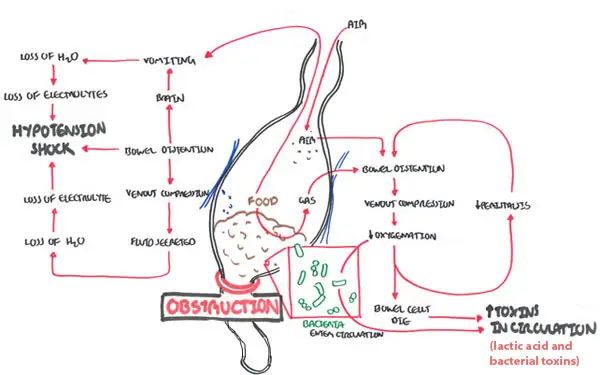
Pathophysiology disruption of the normal flow of intestinal contents leading to proximal dilatation and distal decompression may take 12-24 h to decompress, therefore passage of feces and atus may occur a er the onset of obstruction bowel ischemia may occur if blood supply is strangulated or if bowel wall in ammation leads to venous congestion bowel wall edema and disruption of normal bowel absorptive function can lead to increased intraluminal uid and transudative fluid loss into peritoneal cavity, electrolyte disturbances
| Video: Bowel Obstruction Overview |
Is it a partial or complete bowel obstruction?
- Partial Obstruction - still can pass gas +/- diarrhoea
- Complete Obstruction - can not pass gas or poo
Is it obstruction of the small or large bowel?
| DIFFERENCE BETWEEN SMALL AND LARGE BOWEL OBSTRUCTION | |||
| Small Bowel | Large bowel | Ileus | |
| Main Aetiology (in order) | Adhesions, Hernia, Cancer | Cancer, Diverticulitis, Volvulus | Post operative, medication, chronic disease |
| Nausea,vomiting | Early, may be bilious | Late may be faeculent | Present |
| Abdominal Pain and Distension | Colicky and slight distention + | Colicky and distended ++ | Minimal or absent |
| Constipation | + | + | + |
| Bowel Sounds | Normal, initially increased and may decrease late | Normal, initially increased and may decrease late | Decreased or absent |
| Abdominal X-ray |
|
|
|
| Remember Ileus is temporary paralysis of the myenteric plexus. Contents of the small intestine are acutely unable to transit because of impermanent neural or muscular inadequacy. |
Mechanical obstruction or ileus?
Mechanical Obstruction
- Volvulus
- Intersussception
- Colon Cancer
- Hernia
- Adhesions
- Diverticulitis
Pseudo-obstruction (non-mechanical obstruction)
| Remember Pseudo-obstruction refers to intestinal dysmotility syndromes that have signs, symptoms, and the radiologic appearance of obstruction in the absence of a mechanical cause |
- Ileus Temporary paralysis of the myenteric plexus. Contents of the small intestine are acutely unable to transit because of impermanent neural or muscular inadequacy. Sudden and severe pain, nausea, vomiting, abdominal distention, and inability to tolerate a diet or to pass stools typically accompany ileus, but ultimately the condition resolves completely.
- Toxic Megacolon - defined by a diameter of the rectosigmoid region or descending colon on abdominal plain film of greater than 6.5 cm; an ascending colon diameter of greater than 8 cm; or a cecal diameter greater than 12 cm. Megacolon can be caused by aganglionosis (Hirschsprung’s disease), can be idiopathic (complicating chronic constipation of any cause), or may be a manifestation of a generalized GI dysmotility (intestinoparesis).
- Ogilvie's Syndrome - "acute colonic pseudo-obstruction" It is characterized by acute massive colon dilatation that involves primarily the right side of the colon and is unexplained by mechanical cause. It is most often diagnosed in hospitalized, debilitated, medical or surgical patients with a wide array of medical condition
- Hirschsprung’s disease - (Paediatrics) The most common cause of congenital megarectum and megacolon.
- Chronic Pseudo obstruction - Many causes. Can be divided into Primary (Amyloidosis, myopathies/neuropathies) and Secondary (endocrine disorders, medications and infections)
Absence or presence of intestinal ischemia (simple or strangulated)
- Simple: one obstructing point and no vascular compromise
- Strangulated: Blood supply is compromised and the patient is more ill than you would expect. Features suggesting strangulation are:
- Change in character of pain from colicky to continuous
- Tachycardia
- Pyrexia
- Peritonism
- Bowel sounds absent or reduced
- Leucocytosis
- Raised C-reactive protein (CRP)
Radiography
| X-RAY DIFFERENCES OF SMALL AND LARGE BOWEL | ||
| Small bowel | Large bowel | |
| Location | Central | Peripheral |
| Content | Fluid and air | Faecal matter |
| Wall Patern | Encircling valvulae conniventes visible depending on degree of air filling/distention. | Haustral folds interspaced with Plicae semilunaris |
| Size | 3cm diameter | 6cm diameter (caecum 9cm) |
| 3, 6, 9 Rule |
| Small intestine 3cm |
| Large intestine 6cm |
| Caecum 9cm |
| Remember Any increase in these numbers signify dilatation most likely due to an obstruction |
Management
- Preoperative
- Nil by mouth
- IV fluids
- IV analgesia (pain)
- IV antibiotics
- Nasogastric tube
- Gastric aspiration by means of nasogastric suction (decompression)
- Surgical
- Bowel resection














