

Liver Cirrhosis Complications
Portal Hypertension
Overview
Normal portal vein pressure is 5–10mmHg. Portal hypertension develops when the portal pressure is greater than 12mmHg.
Mechanism of disease
- Increased Intrahepatic resistance of blood flow through the liver due to cirrhosis
- Increased splanchnic blood flow secondary to vasodilation leading to increased portal flow through liver
Cirrhosis is the most common cause of portal hypertension.
Portal Vein Anatomy
- The portal vein drains blood from the GIT so that nutrition absorbed can first enter the liver
- Portal vein is formed from the superior mesenteric vein and splenic vein
- Portal vein ← Superior mesenteric vein + Splenic vein
- Splenic vein ← inferior mesenteric vein
| CAUSES OF PORTAL HYPERTENSION | ||
| Prehepatic | Hepatic | Posthepatic |
| Portal Vein thrombosis | Cirrhosis | Budd-Chiari Syndrome |
| Splenic Vein thrombosis | Acute hepatitis | Constrictive pericarditis |
| Massive splenomegaly | Parasitic – Schistomosis | Tricuspid Regurgitation |
Complications of Portal Hypertension
- Gastroesophageal varices
- Portal Hypertensive gastropathy
- Splenomegaly
- Ascites
- Treat complications above
- Tranjugular Intrahepatic portosystemic shunt (TIPS)
- Liver transplantation (definitive)
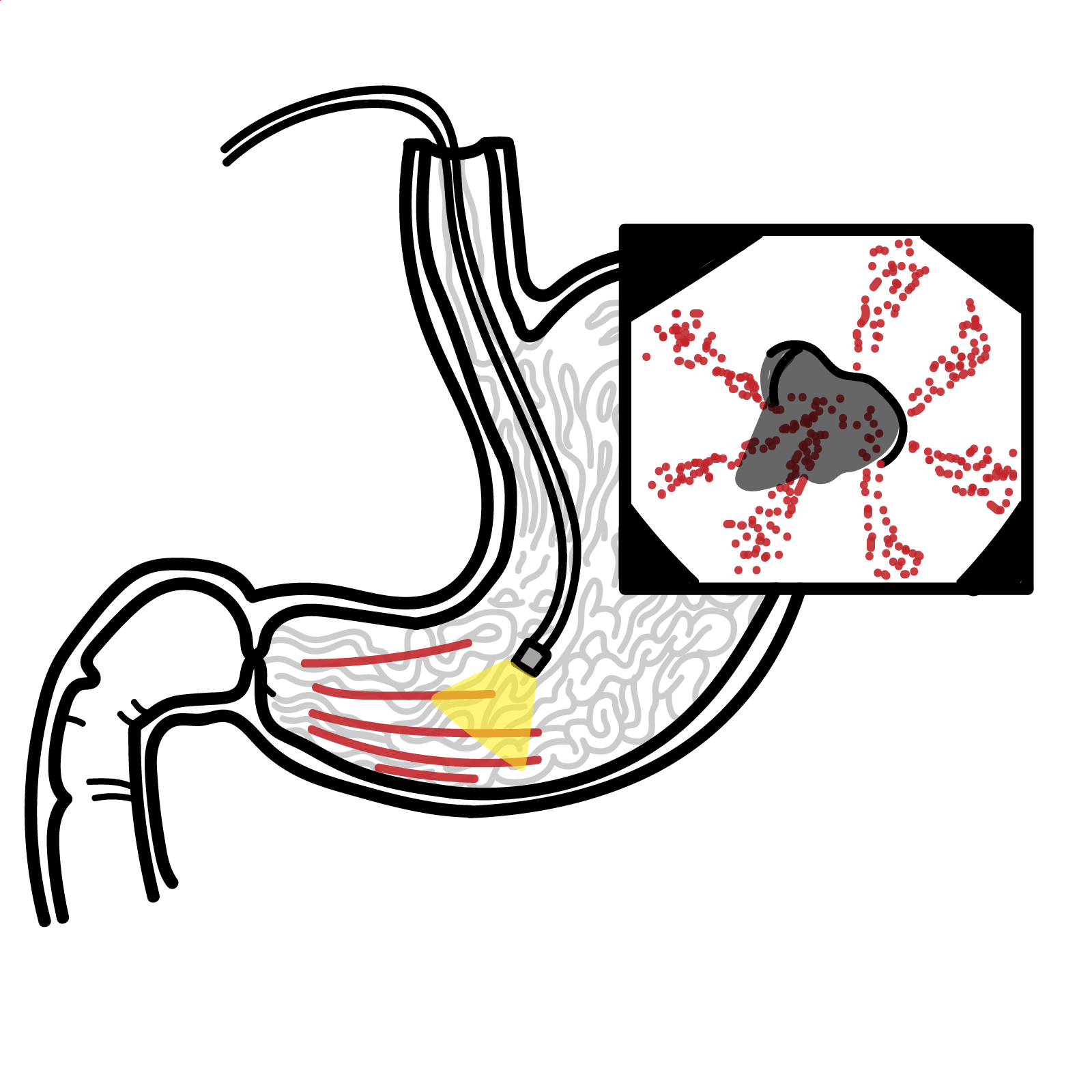
Oesophageal-gastric varices
Overview
>75% of patients with cirrhosis will eventually develop varices. Risk of variceal haemorrhage is 5-15% per year, and is related to variceal size. Risk amplified in progressive CPS and presence of red wale marks. Without secondary prophylaxis, re-bleeding occurs in 60-70%, usually within the first 2 years of index bleed. Screening is important.
Mechanism of disease
Varceal haemorrhage results from rupture of the variceal wall due to excessive wall tension. Tension opposes the variceal transmural pressure, which depends upon portal pressure and vessel size . Once variceal wall rupture occurs, the amount of bleeding is mainly related portal pressure.
Major complication of cirrhosis and portal hypertension is gastroesophageal varices with haemorrhage.
- Gastroscopy
- CT abdo
- MRI abdo
Management of varices
- Prevention – Screening those at risk with gastroscopy
- yearly – small varices
- 2nd yearly – no varices
- If high risk bleeding (Medium and large varices, Any size with red wale markings):
- Betablockers – Propranolol (to reduce portal venous pressure) OR
- Endoscopic variceal band ligation
Pharmacology
Non-selective BetaBlocker (propranolol) – mechanism of action – Reduction in cardiac output and splanchnic blood flow. It allows unopposed alpha-1 adrenergic receptor activity which results in splanchnic vasoconstriction and reduction in portal pressure.
Acute management of variceal bleed – emergency
- Resuscitation
- Bloods – cross match (aim Hb >70)
- Monitor
- Fluid resuscitation
- Contact gastroenterological/surgical team for emergency gastroscopy
- IV Proton pump inhibitors
- IV Somatostatin OR octreotide
- Consider giving vitamin K and fresh frozen plasma to correct clotting problems
- Antibiotics – oral norfloxacin OR IV ciprofloxacin
- Balloon tamponade – for those who can not get endoscopy immediately
- Endoscopy – first line
- Repeated sclerotherapy injection
- Endoscopic variceal band ligation
- Tranjugular Intrahepatic portosystemic shunt (TIPS)
Pharmacology
Octreotide is synthesised somatostatin used to treat acromegaly, portal hypertension and reduces side effects of chemotherapy. It is used in acute oesophageal bleed because it is through to cause vasoconstriction of splanchnic circulation.
Ascites
Overview
Ascites is accumulation of fluid within the peritoneal cavity. Usually 1-2L of fluid in abdomen before patient is aware of abdominal distention.
| Causes of Ascites |
| Portal Hypertension (Cirrhosis main cause) |
| Malignancy |
| Infection |
- Abdominal distention
- Shortness of breath
- Hepatic hydrothorax
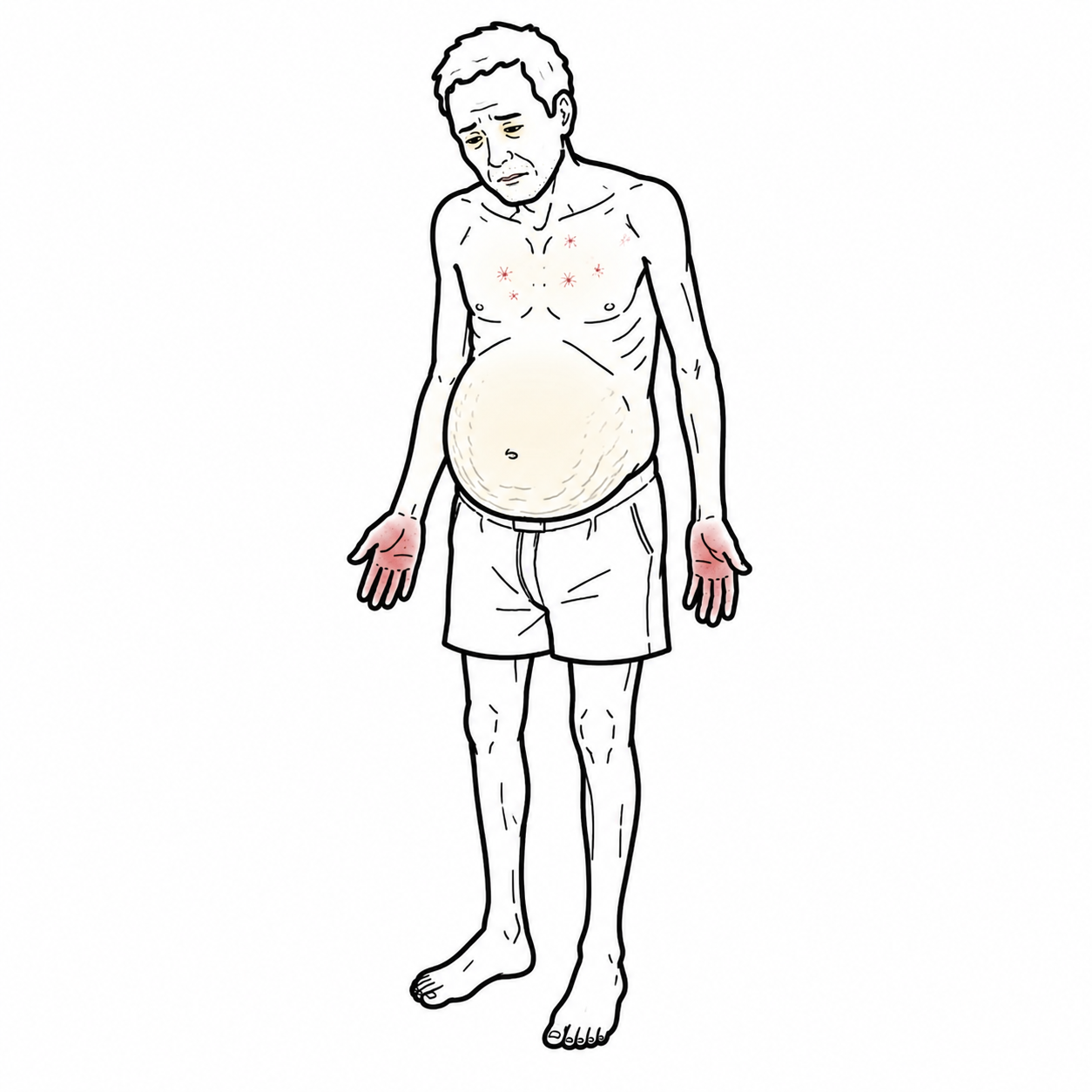
- Malnourished
- Muscle wasting
- Fatigue and weakness
Investigation
Serum to albumin gradient (SAAG)
- >11 – portal hypertension
- <11 – malignant or infectious
Management
- Aim 500g of weight loss/day
- Sodium restriction
- Lactulose
- Spironolactone
- If Urinary K+ >1 = 150mg/day
- If Urinary K+ <1 can give more.
- Frusemide
- Paracentesis +IV albumin replacement
- TIPS (refractory ascites – not improving with diuretics)
Complication
- Spontaneous bacterial peritonitis
- Spironolactone associated hyperkalaemia
Paracentesis with high neutrophil count >250 is highly suspicious of spontaneous bacterial peritonitis.
Spontaneous Bacterial Peritonitis (SBP)
- Common complication of ascites
- Usually asymptomatic
- 25% mortality
- E-coli main causative agent
- Paracentesis with high neutrophil count highly suggestive of SBP
- Treatment: cephalosporin or Pip/taz
- Primary prophylaxis in those with low protein (<10g/L) ascites or bilirubin >50 with impaired renal function
Splenomegaly
Clinical features
- Enlarged spleen
- Thrombocytopaenia and leukopaenia
Complications
- Hypersplenism
Click here for more information on splenomegaly
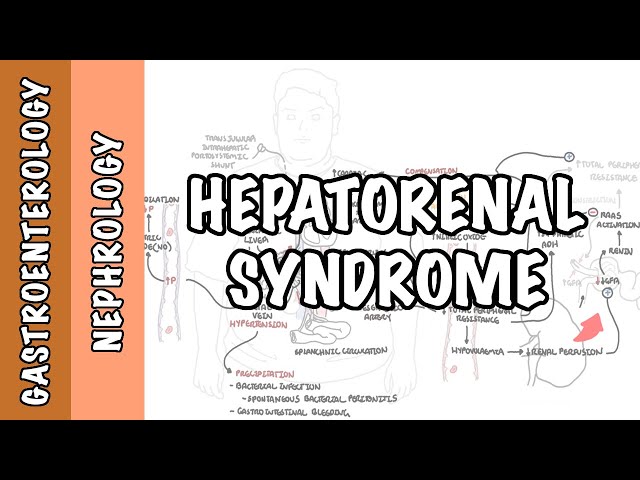
Hepatorenal syndrome
Overview
- Renal failure without renal pathology due to renal vasoconstriction
- Renal vasoconstriction leads to RAAS activation which further causes systemic vasoconstriction
- Vasodilatation in splanchnic system
- Large Ascites
- High creatinine
Types of Hepatorenal syndrome
- Type I – decrease eGFR and increase in creatinine within 1-2 weeks of presentation
- Type II – decrease eGFR with increase in creatinine level but stable
Management
- Midodrine
- α-agonist
- Octreotide
- IV albumin
- Liver transplantation
Pharmacology
Midrodrine is a α1-receptor agonist and exerts its actions via activation of the alpha-adrenergic receptors of the arteriolar and venous vasculature, producing an increase in vascular tone and elevation of blood pressure.
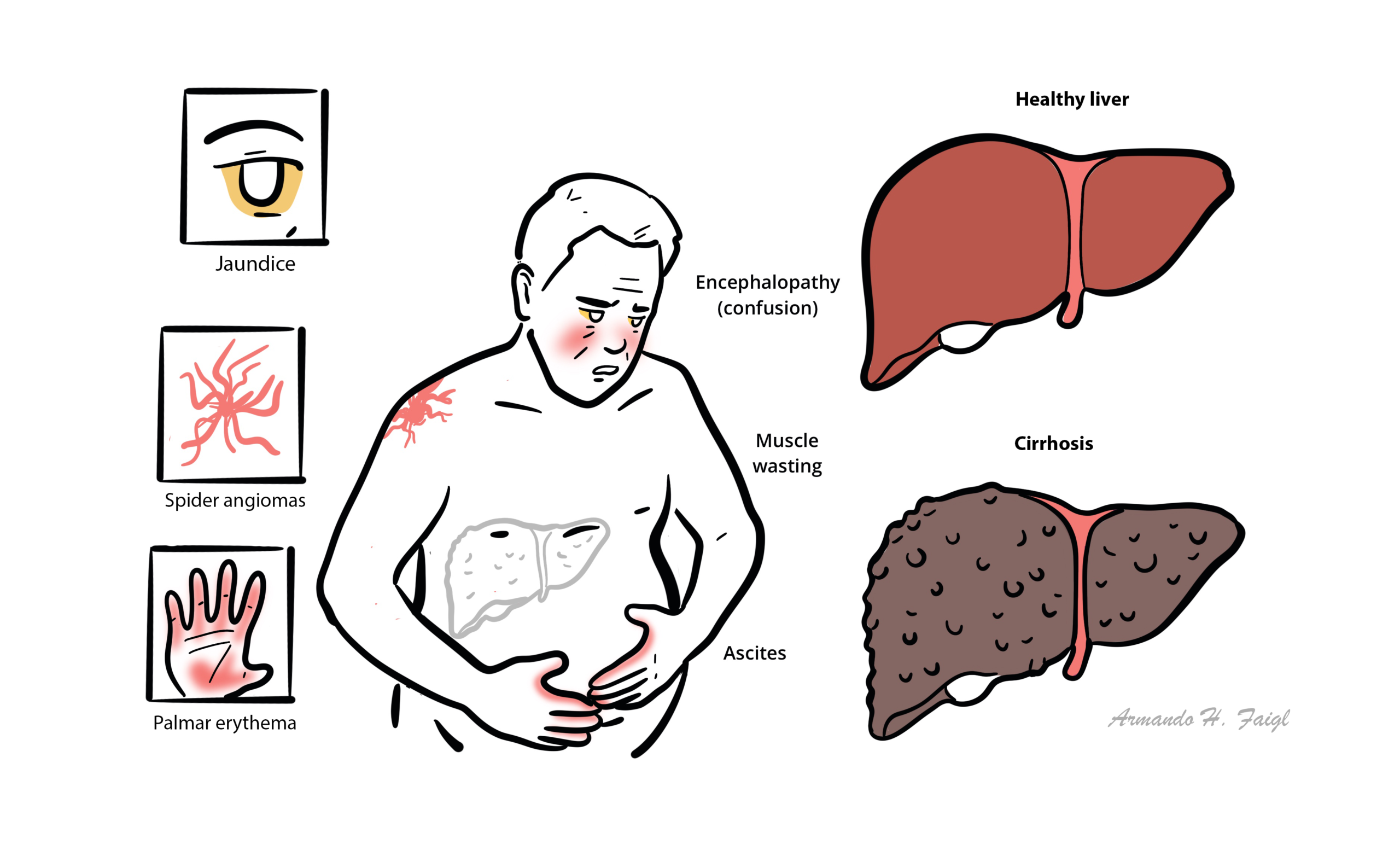
Hepatic encephalopathy
Overview
- Alteration in mental status and cognitive function due to liver failure
- Clinical diagnosis
Precipitating events
- Hypokalaemia
- Infection
- Increased dietary protein load
- Electrolyte disturbances
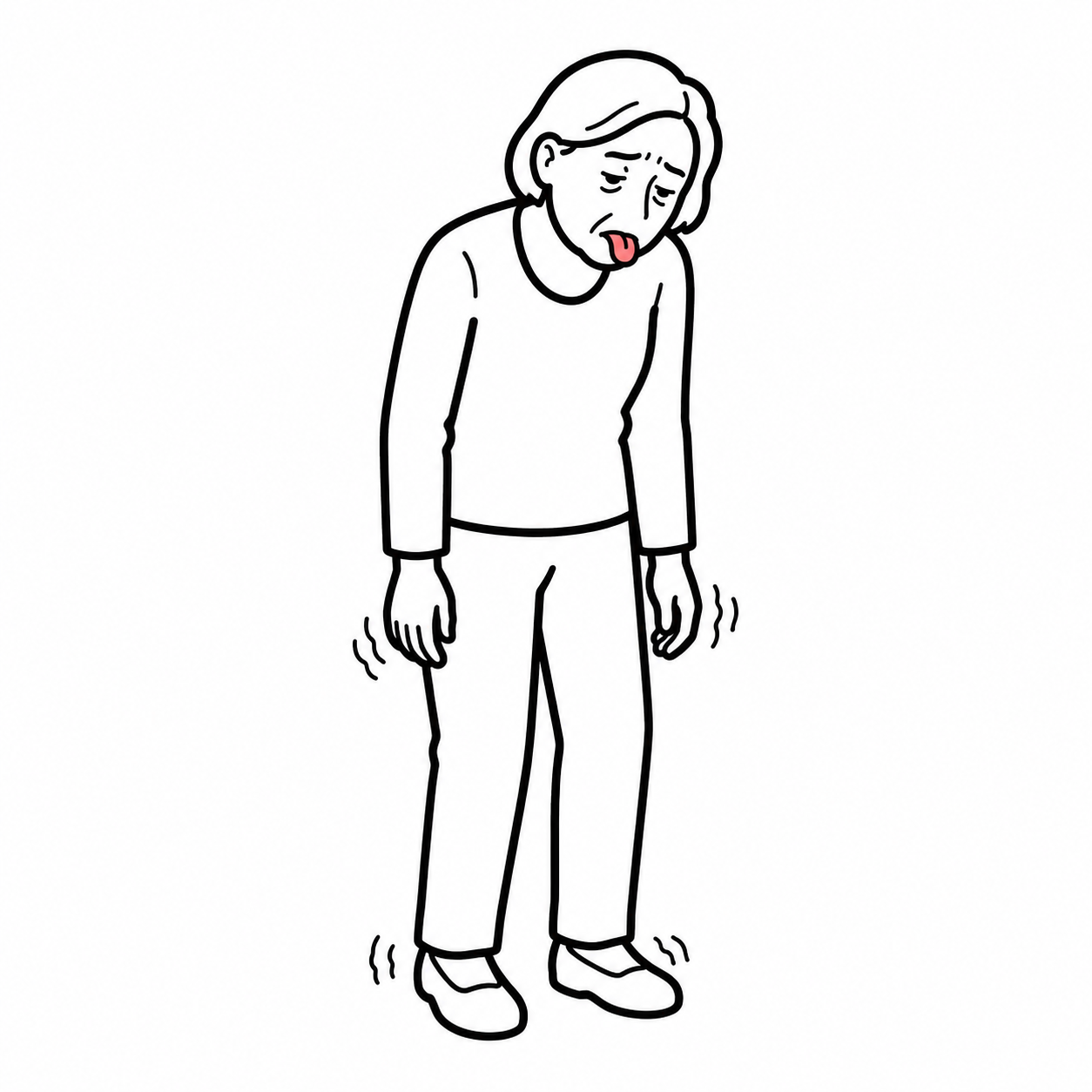
Clinical features
- Personality change within weeks to months
- Violent OR
- Sleepy
- Ascites
- Asterixis
Mechanism of condition
- Gut-derived neurotoxins bypass liver
- Neurotoxins reach the brain
Investigations
- Ammonia (does not correlate with severity)
Management
- Identify precipitating factor and correct it
- Lactulose OR antibiotics (for those where lactulose is no good) – to promote 2-3 soft stools a day and minimise ammonia production by gut bacteria
- Zinc supplementation
Other complications
Bone disease due to Vitamin D deficiency
- The liver plays a role in the conversion of cholecalciferol to calcidiol
- Calicidiol then goes to kidneys to become calcitriol the active form of vitamin D
- Liver failure means the conversion from cholecalciferol to calcidiol does not occur so there is vitmain D deficiency
- Vitamin D deficiency leads to hypercalcaemia
Liver Transplantation
Indications for chronic liver disease
- Life threatening complications
- MELD score >15
- 2 year mortality of 50% without transplant
- Diuretic resistant ascites
- Recurrent hepatin encephalopathy
- Recurrent CBP
- Recurrent or persistent gastrointestinal haemorrhage
- Intractable cholnagitis
- Hepatorenal syndrome
| MELD SCORE Stratifies severity of end-stage liver disease, for transplant planning. | |
| Factors: Dialysis, bilirubin, INR, Sodium | |
| MELD SCORE | Mortality rate (3-month) |
| <9 | 3% |
| 10-19 | 15% |
| 20-29 | 30% |
| 30-39 | 60% |
| >40 | >70% |
Stratifies severity of end-stage liver disease, for transplant planning.
Acute liver disease (King’s College Hospital Criteria)
- Paracetamol induced liver failure
- arterial pH <7.3 OR
- all three of the following: INR >6.5, Serum creatinine >300 and Grade III/IV encepalopathy
- Non-paracetamol induced acute liver failure
Liver Transplantation of hepatocellular carcinoma (Milan Mazzaferro criteria)
- A single nodule <5cm OR
- 3 nodules the largest of which is <3cm
- no evidence of gross vascular invasion
- No metastasis
- 4 year survival of 75%







Members only discussions coming soon…