

Acute Cholecystitis

Overview
Acute cholecystitis is acute inflammation of the gallbladder, usually caused by a gallstone obstructing the cystic duct. Persistent obstruction causes gallbladder distension, inflammation and possible secondary bacterial infection. Most cases are calculous, while acalculous cholecystitis occurs mainly in critically ill or severely immunocompromised patients.
Definition
Cholecystectomy: surgical removal of the gallbladder.
Calculous cholecystitis: gallbladder inflammation caused by a gallstone or biliary sludge obstructing the cystic duct.
Acalculous cholecystitis: gallbladder inflammation without stones, usually associated with critical illness, gallbladder stasis and ischaemia.
Murphy sign: arrest of inspiration because of pain when the examiner palpates the right upper quadrant.
Empyema of the gallbladder: accumulation of infected pus within the gallbladder.
Aetiology & Risk Facotrs
Calculous cholecystitis
Risk factors are similar to those for gallstone formation:
- Increasing age
- Female sex
- Obesity or metabolic syndrome
- Pregnancy
- Rapid weight loss
- Family history of gallstones
- Diabetes
- Haemolytic disorders
- Ileal disease or resection
- Certain medicines, including ceftriaxone
Acalculous cholecystitis
Associated with:
- Critical illness or sepsis
- Major trauma or burns
- Prolonged fasting or total parenteral nutrition
- Major surgery
- Mechanical ventilation
- Severe immunosuppression
- Gallbladder ischaemia or impaired emptying.
Pathophysiology
- A gallstone becomes lodged in the gallbladder neck or cystic duct.
- Continued bile secretion causes gallbladder distension and increased intraluminal pressure.
- Reduced venous and lymphatic drainage causes gallbladder-wall oedema and ischaemia.
- Chemical inflammation develops, followed by possible secondary bacterial infection.
- Untreated inflammation may progress to gangrene, empyema, perforation or peritonitis.
Clinical Manifestation
- Persistent right upper-quadrant or epigastric pain, usually lasting longer than 4–6 hours
- Pain may radiate to the right shoulder or back
- Fever
- Nausea and vomiting
- Anorexia
- Symptoms may follow a fatty meal
Biliary colic usually resolves within hours; persistent pain with fever and Murphy sign suggests acute cholecystitis.
Clinical examination
- Right upper-quadrant tenderness
- Positive Murphy sign
- Fever
- Tachycardia
- Guarding or a palpable tender gallbladder in some patients
- Jaundice is uncommon and should raise concern for:
- Common bile-duct obstruction
- Cholangitis
- Mirizzi syndrome
- Another hepatobiliary disorder
Older adults, patients with diabetes and immunocompromised patients may have minimal pain or fever despite severe disease.
Courvoisier’s Law: The presence of jaundice, palpable gallbladder means that the jaundice is unlikely to be due to stones. It is tumour of the head of the pancreas until proven otherwise.
- Appendicitis
- Acute pancreatitis (can be due to gallstones)
- Pyelonephritis
- Hepatic abscess
- Hepatic tumour
- Gonococcal or chylamdial perihepatitis
Marked jaundice or significantly abnormal cholestatic LFTs suggest common bile-duct obstruction or cholangitis rather than uncomplicated cholecystitis.
Diagnosis
Diagnosis is based on a combination of:
- Local inflammatory features: right upper-quadrant pain, tenderness or Murphy sign
- Systemic inflammation: fever, elevated white-cell count or raised CRP
- Imaging findings consistent with acute cholecystitis
No single clinical sign or laboratory test is sufficiently accurate alone.
- FBC: leukocytosis or neutrophilia
- CRP: usually elevated
- LFTs: often normal or mildly abnormal
- Bilirubin and ALP may rise with common bile-duct obstruction
- UEC and creatinine: dehydration and preoperative assessment
- Lipase: exclude gallstone pancreatitis
- Blood cultures if septic, hypotensive, delirious or at risk of resistant infection.
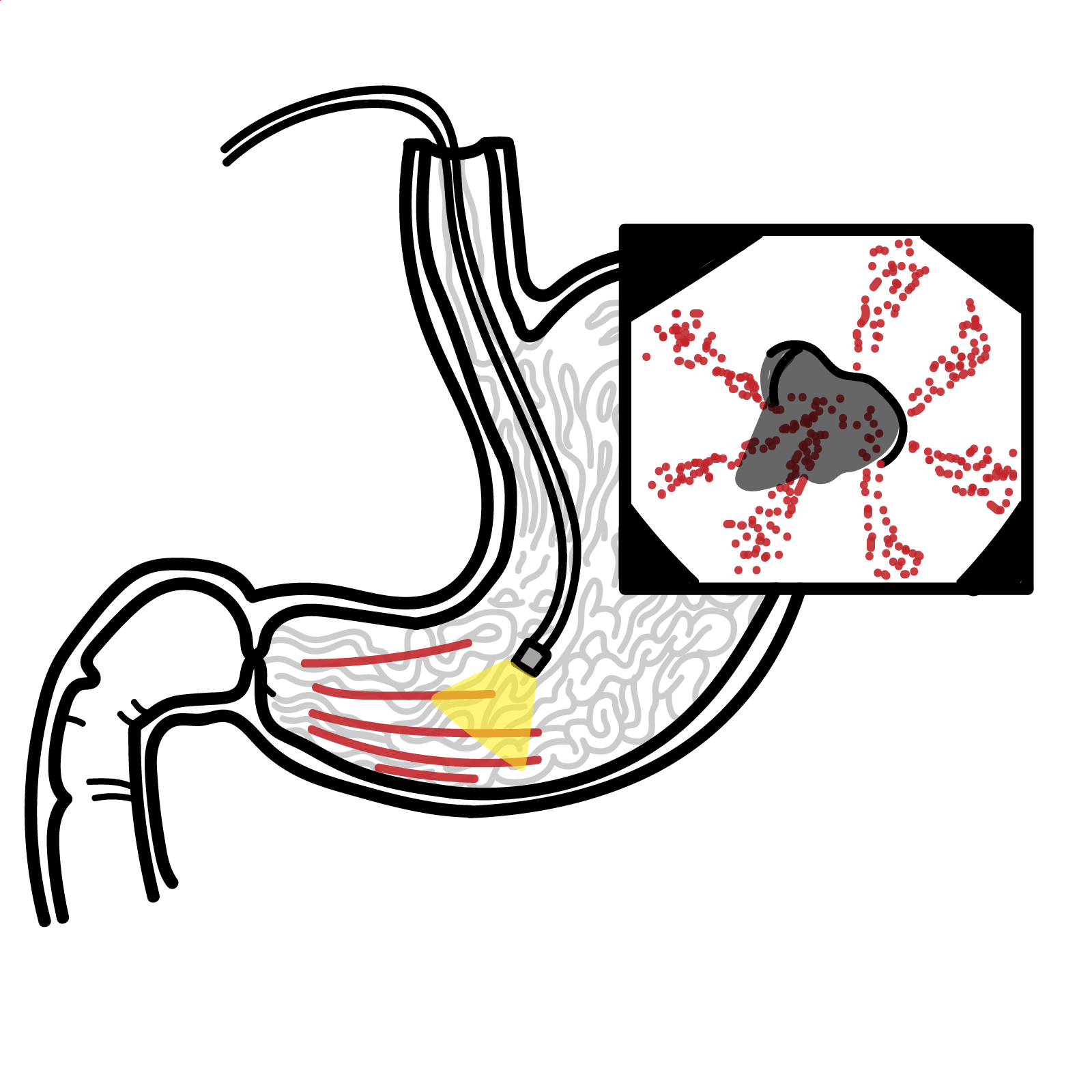
Abdominal ultrasound — first-line
Ultrasound is the preferred initial imaging test because it is widely available, non-invasive and effective at detecting gallstones.
Further imaging
- HIDA scan: failure of the gallbladder to fill suggests cystic-duct obstruction; useful when ultrasound is inconclusive.
- CT abdomen: useful for alternative diagnoses and complications such as gangrene, emphysematous change, abscess or perforation.
- MRCP: assesses suspected common bile-duct stones without using invasive instrumentation.
- Endoscopic ultrasound: may detect small common bile-duct stones when MRCP is inconclusive.
On ultrasound findings suggestive of an ultrasound echogenic focus (dense) and acoustic shadow.
Treatment
Initial management
- Hospital assessment
- Nil by mouth initially
- IV fluids and correction of electrolyte abnormalities
- Analgesia, commonly NSAID or opioid therapy as appropriate
- Antiemetics
- Monitor vital signs, urine output and signs of sepsis
- IV antibiotics covering common enteric gram-negative organisms ± anaerobes according to illness severity, allergy history, local resistance and hospital guidelines.
Definitive treatment
- Early laparoscopic cholecystectomy is the preferred definitive treatment for most patients fit for surgery.
- It should be performed during the index admission and as soon as practical.
- WSES recommends surgery within seven days of admission and within ten days of symptom onset when appropriate expertise is available.
- Early surgery reduces total hospital stay and recurrent gallstone-related complications compared with delayed treatment.
Patient unsuitable for immediate surgery
- Conservative treatment with IV fluids, analgesia and antibiotics may be used temporarily.
- Percutaneous cholecystostomy: image-guided drainage of the gallbladder for patients with sepsis who are not suitable for surgery.
- Endoscopic ultrasound-guided gallbladder drainage may be considered at experienced centres.
- Interval cholecystectomy should be considered if the patient later becomes fit for surgery because recurrence is common without definitive removal.
Suspected common bile-duct obstruction
- MRCP or endoscopic ultrasound may be used to investigate.
- ERCP is indicated for common bile-duct stones causing obstruction or associated acute cholangitis.
Complications & Prognosis
Complications
- Gallbladder empyema
- Gangrenous cholecystitis
- Gallbladder perforation
- Pericholecystic or intra-abdominal abscess
- Biliary peritonitis
- Sepsis and septic shock
- Emphysematous cholecystitis, particularly in patients with diabetes
- Cholecystoenteric fistula
- Gallstone ileus
- Mirizzi syndrome
- Recurrent cholecystitis
- Common bile-duct stones, cholangitis or gallstone pancreatitis
- Surgical complications:
- Bile-duct injury
- Bile leak
- Bleeding
- Infection
- Retained bile-duct stones.
- Prognosis is generally excellent when acute cholecystitis is recognised early and treated with laparoscopic cholecystectomy.
- Delayed treatment increases the risk of gangrene, perforation, abscess and sepsis.
- Conservative treatment without cholecystectomy carries a significant risk of recurrent gallstone-related symptoms and later hospitalisation.
- Prognosis is poorer in older adults and patients with associated complications above
References
- Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculous cholecystitis. World J Emerg Surg. 2020;15:61. doi:10.1186/s13017-020-00336-x.
- Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018;25(1):41–54. doi:10.1002/jhbp.515.
- Gallaher JR, Charles A. Acute cholecystitis: a review. JAMA. 2022;327(10):965–975. doi:10.1001/jama.2022.2350.
- Bonomo RA, Chow AW, Edwards MS, et al. 2024 clinical practice guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation. Clin Infect Dis. 2024. doi:10.1093/cid/ciae346.
- National Institute for Health and Care Excellence. Gallstone disease: diagnosis and management. Clinical guideline CG188. London: NICE; 2014.






Members only discussions coming soon…