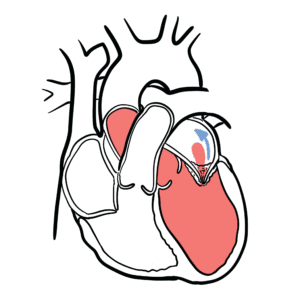
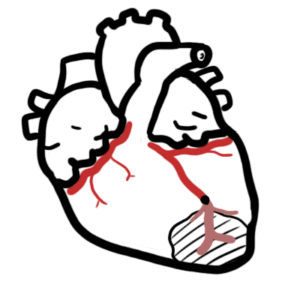
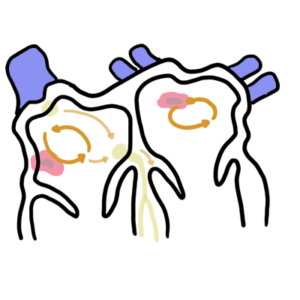
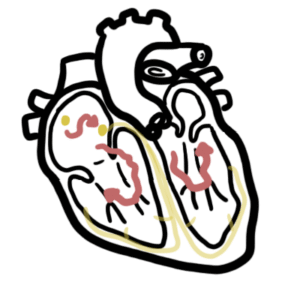
0:00 In this video we're going to talk about aortic stenosis. 0:07 This is an overview and introduction. 0:10 Aortic stenosis is characterized by obstruction of the left ventricular outflow 0:15 , resulting 0:16 in the decrease in cardiac output. 0:20 Aortic stenosis can be mild to moderate and is usually asymptomatic, but it is 0:26 always 0:27 important to monitor this stenosis that occurs in the aorta. 0:32 All the valves of the heart can be heard most prominently in certain areas 0:37 across 0:38 our thorax. 0:40 The aortic valve is best heard in the right second intercostal space, perist 0:46 ernal. 0:47 The pulmonary valve left second intercostal space, peristernal. 0:52 The tricuspid valve left fourth intercostal, peristernal. 0:57 And then the mitral valve left fifth intercostal space mid-provicular. 1:07 The pulmonary valve is made up of three leaflets. 1:09 The mitral valve two leaflets. 1:12 The tricuspid valve three leaflets. 1:14 And the aortic valve three leaflets as well. 1:18 And of all the heart valves, the mitral is normally the only valve with two 1:23 leaflets, 1:23 and that is why it is also called bicuspid. 1:28 During the cardiac cycle, when the aortic valve is open, the pulmonary valve is 1:33 open 1:33 as well. 1:35 And when both these valves are open to pump blood out of the heart, the tricusp 1:40 id and 1:40 mitral valve close. 1:43 This is what a normal aortic valve looks like when it's opened and when it's 1:54 closed. 1:55 The heart with a stenotic valve cannot pump blood efficiently. 2:00 Here is an open and closed aortic valve with stenosis. 2:05 Even when the aortic valve is open, the stenosis results in a decreased blood 2:11 flow. 2:12 With decreased blood flow, there is decreased cardiac output. 2:18 Because of the decreased in cardiac output, we get the following three cardinal 2:22 signs and 2:22 symptoms of aortic stenosis. 2:25 These are dizziness or syncope on exertion, dyspnea on exertion, and exertional 2:37 angina. 2:39 In examination we can feel a slow rate of rise of the carotid arteries, which 2:44 can be 2:44 felt around the neck. 2:47 Normally, the carotid pulse rises fast, but in aortic stenosis the carotid 2:53 pulse is slow 2:55 and weak. 2:58 On oscillation of the right second intercostal space, we have reduced intensity 3:05 of the second 3:07 hot sound, which is the sound when the aortic and pulmonary valve close. 3:13 Drawing it out here, we normally have two hot sounds, S1 and S2. 3:20 S1 is your AV valve closing, which are your tricuspid and mitral valves. 3:27 And S2 is when your aortic and pulmonary valves close. 3:34 We are listening to the right second intercostal space murmur in aortic sten 3:39 osis, but first 3:40 looking at the normal. 3:43 We have a first hard sound and then a second hot sound. 3:47 Drawing these sounds out, we can divide it into three things. 3:52 S1 is when your AV valves close, and your blood is in the ventricles. 3:59 The ventricles begin to contract. 4:03 In S1 and S2, your ventricles are contracting so hot that it pushes blood 4:09 through the aortic 4:11 valve. 4:13 S2, your aortic valve, closes again, allowing the ventricles to fill back with 4:22 blood. 4:23 Thus, we can say that between S1 and S2 is cystly, when the ventricles are 4:30 contracting, 4:32 and from S2 to S1 is diastole, when the ventricles are relaxed and filled back 4:41 with blood. 4:41 In aortic stenosis, the murmur we hear begins at S1, when the atrial vent 4:47 ricular valve closes. 4:50 And then we hear the aortic valve open. 4:53 The blood is being squeezed through the aortic valve slowly. 4:58 And so we get this greater turbulent flow until the ventricles relax again, and 5:04 the aortic 5:05 valve closes. 5:08 We call the aortic stenosis murmur a systolic clique crescendo decrescendo mur 5:14 mur, or ejection 5:16 systolic murmur. 5:18 Again, the AV valve closes, ejection clique as the aorta valve opens, 5:26 turbulence through 5:28 the aortic valve increases, then decreases, and then the aortic valve closes. 5:34 It is important to know that this murmur can radiate through the carotids. 5:45 There are three major etiologies of aortic stenosis. 5:49 One is congenital abnormal valve, a unicuspid or bicuspid aortic valve. 5:56 Two, calcification of the aortic valve usually with age. 6:01 And three, a rheumatic valvular heart disease. 6:07 Here is an abnormal aortic valve, which is bicuspid. 6:11 Here is a calcified aortic valve resulting in stiffening. 6:16 A rheumatic valve forms scar tissue leading to stenosis. 6:24 Conditions include an ECG, which may show left ventricular hypertrophy. 6:28 Cardiac catheterization can be performed through the femoral artery or radial 6:34 artery, 6:35 where the catheter is fed through till it reaches the aortic valve. 6:44 Here is a catheter approaching the aortic valve. 6:48 The catheter allows visualization of the aortic valve. 6:53 Restoracic echocardiogram can also be performed and is gold-standard for 6:57 looking at valvular 6:59 heart diseases. 7:02 Management of aortic stenosis includes surgical valve replacement, or repair. 7:08 A valve replacement can be mechanical or bioprosthetic. 7:12 There are weaknesses and strengths between the two. 7:16 Mechanical valve replacement is often used for the younger people because it 7:20 lasts longer. 7:22 Use of short, long-term anticoagulants and antibiotics may be necessary 7:26 following surgery 7:28 for those who are susceptible to infections and complications. 7:33 For patients unable to undergo a valve replacement, there is a lune valvular 7:38 plastic, where the 7:39 valves foramen is dilated. 7:42 And transcatheter valve replacement can also be performed following a balloon 7:47 valvular 7:47 plastic.