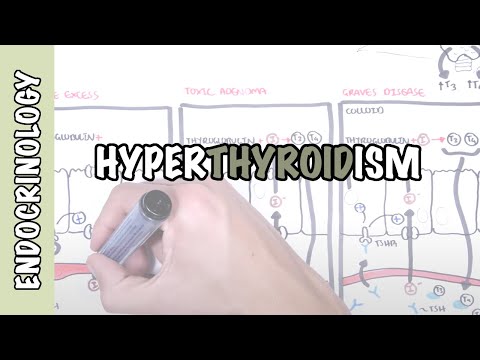
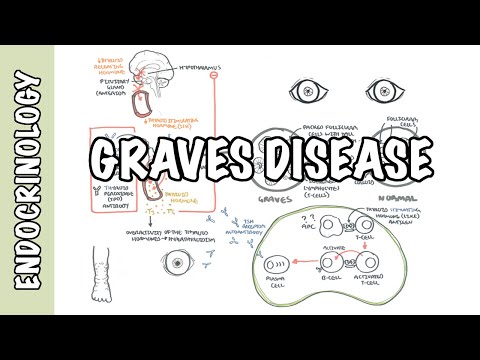
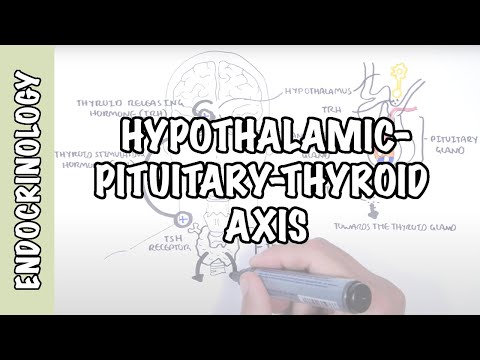
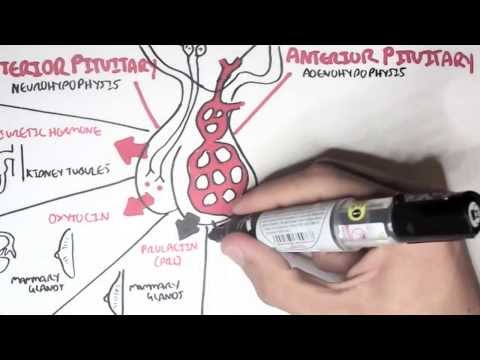
0:00 Hello, in this video we're going to talk about thyroid nodules. 0:07 A thyroid nodule is technically a goiter, which means an enlarged thyroid gland 0:11 . 0:12 A thyroid nodule can be defined as a nodule goiter. 0:15 Thyroid nodule is usually identified by the patient, on routine examination or 0:20 incidentally 0:21 on imaging such as a CT neck or CT chest. 0:25 When someone notices a lump on their neck or thyroid, I guess one of the most 0:28 concerning 0:28 things is could this be cancer? 0:31 Majority of thyroid nodules are benign. 0:34 Thyroid cancer make up about 5% of the cases, and their fact is that increases 0:39 the suspicion 0:40 of cancer, such as if the thyroid nodule is in children, young adults, a person 0:46 with 0:46 a history of radiation to the neck or head, and also someone who has a family 0:50 history 0:51 of thyroid cancer. 0:54 A thyroid nodule is very common, 50% of the population have it, but only 10% 0:59 can actually 1:00 be felt. 1:02 Like all thyroid diseases, it is more common in women, and the incidence 1:06 increases with 1:07 age. 1:09 Majority of thyroid nodules, as we discussed, are benign, 95% of cases. 1:14 Some common examples of benign thyroid nodules are thyroid adenoma, which can 1:19 be a basic 1:20 benign follicular adenoma, the most common cause of a solitary thyroid nodule. 1:26 Of course this adenoma can undergo mutation in its thyroid stimulating hormone 1:30 receptor, 1:31 and can progress to become a toxic adenoma, which is also benign. 1:36 A toxic adenoma is where the adenoma becomes hyperfunctioning, and produces a 1:42 lot of T3 1:43 and T4 irrespective of thyroid stimulating hormone. 1:48 Another cause of thyroid nodule is toxic multinodular goita. 1:53 As the name suggests, toxic, here again the thyroid nodules have autonomous 1:58 production 1:59 of T3 and T4, it's producing a lot of T3 and T4 irrespective of thyroid 2:03 stimulating hormone. 2:06 A thyroid cyst is another cause of thyroid nodule, and essentially is a fluid 2:10 sac. 2:11 Another cause of thyroid nodule is Hashimoto's thyroiditis, which is an 2:14 autoimmune disease 2:15 characterized by antibodies against thyroid peroxidase and the thyroid gland, 2:21 resulting 2:21 in thyroid damage. 2:23 This inflammation and damage to the thyroid causes the nodules to form. 2:29 5% of thyroid nodules are cancers, and there are many types of thyroid cancer, 2:34 which we 2:35 will not talk about, but the most common thyroid cancer is papillary thyroid 2:40 cancer. 2:41 There are features of the thyroid nodule which may sway one to think that it is 2:44 cancerous, 2:45 and this includes being a non-functional thyroid nodule, meaning the thyroid 2:50 nodule doesn't 2:51 produce any thyroid hormones. 2:54 Another feature of the thyroid nodule can be that if it's an irregularly shaped 2:59 thyroid 3:00 nodule, this also may suggest cancer. 3:04 There are a number of investigations that can be ordered for people with 3:07 thyroid nodules. 3:08 These include thyroid stimulating hormone levels in the blood, thyroid 3:12 ultrasound, a radio-nucleotide 3:14 scan, also known as a thyroid scan, or thyroid centigraphy, there are so many 3:19 names for it. 3:21 A blood test looking at free T3 and T4, and for a definitive diagnosis, a fine 3:27 needle aspiration 3:28 of the thyroid nodule with an ultrasound. 3:31 Because thyroid nodules are so common, not everyone gets a fine needle 3:35 aspiration, and 3:36 there are only specific indications for it. 3:39 In the next part of this video, we will follow an approach to someone who 3:43 presents with a 3:44 thyroid nodule. 3:46 This approach can also be used with someone who has a diffuse goiter as well. 3:51 So we begin with the identification of the thyroid nodule through history and 3:55 of course 3:55 examination. 3:57 Looking at the brain, the hypothalamus produces thyroid trope in releasing 4:02 hormone, TRH, which 4:03 targets the anterior pituitary gland to release thyroid stimulating hormone, TS 4:10 H. 4:10 The thyroid stimulating hormone will then of course target the thyroid gland to 4:14 produce 4:14 T3 and T4. 4:16 The first thing to order with anyone with a thyroid nodule or a thyroid 4:21 pathology is 4:22 thyroid stimulating hormone levels, and a plus minus ultrasound of the thyroid 4:29 gland. 4:30 If the thyroid stimulating hormone level is high or normal, an ultrasound 4:35 should be ordered. 4:37 High thyroid stimulating hormone should raise suspicion of hypothyroidism. 4:42 The ultrasound helps assess the anatomy of the thyroid gland and the nodule, 4:47 and its 4:47 adjacent structures. 4:49 It provides more anatomical detail than the thyroid nucleotide scan. 4:54 The thyroid ultrasound can help identify any suspicious features of cancer. 5:00 Suspicious ultrasound findings include a nodule greater than 1 cm, solid and 5:06 hypoechoic, 5:07 a nodule that is large or rapidly growing, a nodule with micro calcification, a 5:13 nodule 5:13 with central vascularity, a nodule that is taller than it is wider. 5:21 After the ultrasound is done, the next question to ask is, does this thyroid 5:26 nodule meet the 5:26 criteria for a fine needle aspiration? 5:30 The criteria for a final aspiration includes those suspicious findings we just 5:34 talked about 5:34 on ultrasound. 5:35 So if yes, there is suspicious findings on the ultrasound, then a fine needle 5:39 aspiration 5:40 should be performed. 5:42 If there is no suspicious findings and the thyroid nodule does not meet the 5:47 fine needle 5:47 aspiration criteria, then we just monitor the nodule and may repeat a thyroid 5:53 ultrasound 5:54 in a few months time. 5:57 Focusing now on fine needle aspiration, it is essentially where you use a 6:02 needle and 6:03 aspirate the content of the thyroid nodule with the help of the ultrasound. 6:07 The aspiration is sent to the laboratory for psychology to see the cells in 6:13 more detail. 6:15 The fine needle aspiration results are then classified into what is called the 6:19 best Thesda 6:19 classes of which there are six. 6:24 Class one is a non-diagnostic result, which means that probably insufficient 6:29 samples were 6:30 taken. 6:31 In this scenario, it is advised to repeat the fine needle aspiration. 6:35 Class two is benign adenoma. 6:38 Class three is atypia of undetermined significance or follicular of und 6:42 etermined significance. 6:44 In this scenario, it is important to monitor the nodule. 6:48 Four classes four, five and six, which are follicular neoplasia, suspicious for 6:54 malignancy 6:55 and malignancy, a thyroidectomy is advised. 7:00 A thyroidectomy can be partial or complete, which basically means removal of 7:05 part or all 7:06 of the thyroid gland. 7:10 Now to recap, we came down the pathway where there was initially normal or high 7:17 TSH levels. 7:19 Important that people with high TSH, high thyroid stimulating hormones, these 7:24 guys should 7:25 also be screened for causes of hypothyroidism, such as Hashimoto's disease, if 7:32 indicated. 7:33 Now let us follow the algorithm when there is low TSH, low TSH, which is low 7:40 thyroid stimulating 7:41 hormone levels, should ring alarm bells for hyperthyroidism. 7:47 Because remember, high T3 and high T4 will have a negative feedback to reduce T 7:53 SH release. 7:54 When someone has low TSH, the next investigation should be a thyroid centigraph 7:59 y. 7:59 Thyroid centigraphy is also known again as a thyroid radionucleotide scan and 8:03 also known 8:04 as a thyroid scan. 8:07 Iodine is an important component of thyroid hormones. 8:09 A thyroid centigraphy is where a chemical tagged molecule such as iodine is 8:14 given. 8:14 Iodine is taken up by the thyroid gland normally. 8:17 If the thyroid nodule does not take up any iodine, it is non-functional and 8:22 means it 8:23 does not synthesize or produce any thyroid hormones. 8:27 The other side is an autonomous nodule where the nodule is taking up iodine to 8:31 produce 8:32 thyroid hormones. 8:34 When a nodule has uptake of iodine on the thyroid scan, it is called a hot nod 8:40 ule and 8:41 it is rarely cancerous. 8:44 A cold non-functioning nodule on the other hand raises suspicion of thyroid 8:48 cancer and 8:48 should have an ultrasound with consideration of a fine little aspiration for a 8:52 definitive 8:52 diagnosis. 8:55 A hot autonomous nodule can either be taken up way too much iodine than the 8:59 rest of the 9:00 thyroid gland or it is taking up iodine at the same concentration or level as 9:04 the rest 9:05 of the thyroid gland. 9:07 To be exactly sure, it is advised that free T3 and T4 be measured. 9:13 A normal T3 and T4 with low TSH is a clinical diagnosis of subclinical hyperthy 9:22 roidism. 9:24 A clinical hyperthyroidism will require monitoring because subclinical hyperthy 9:28 roidism can evolve 9:30 and become hyperthyroidism. 9:33 A high T3 and T4 with low TSH means hyperthyroidism. 9:40 The nodule is responsible for producing excess T3 and T4. 9:46 And because this is a nodule and it is taking up a lot of iodine on the scan, 9:51 it is likely 9:52 to be a toxic adenoma. 9:59 Toxic adenoma is either managed by surgery, a thyroidectomy or by radioactive 10:05 iodine. 10:06 In this treatment, radioactive iodine is given, which will be mostly taken up 10:11 by the hyperactive 10:13 autonomous nodule. 10:15 The radioactive iodine will break down, omitting radioactive waves, destroying 10:22 the tissue, thus 10:23 hopefully shrinking the thyroid nodule or making it less functional. 10:28 So we just looked at an approach to a thyroid nodule and this same approach can 10:32 be used 10:33 for someone with a diffuse goiter. 10:36 I hope this video was helpful, thank you for watching. 10:45 You