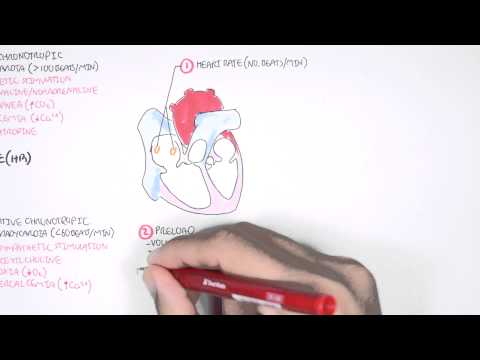
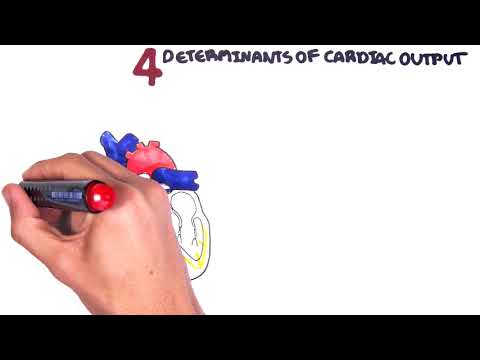
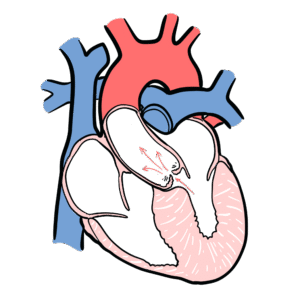
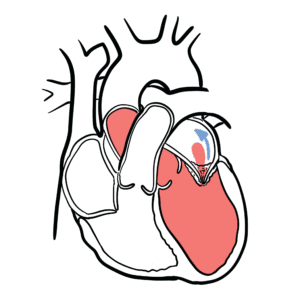
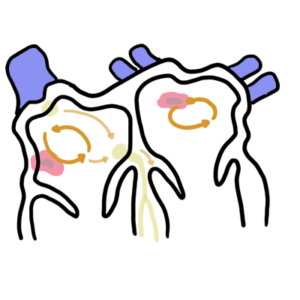
0:00 Hello. In this video, we're going to talk about mean arterial pressure and its 0:10 relationship 0:11 with other factors such as your cardiac output. So here we have a diagram of 0:17 the heart. Now, 0:18 two factors are used to calculate your cardiac output. These are your heart 0:21 rate, which is 0:22 your conduction system and your stroke volume, the amount of blood ejected by 0:27 the heart with 0:29 each beat. So heart rate, stroke volume, give your cardiac output. But there 0:33 are other three 0:34 things that influence your stroke volume. This is your preload, contractility 0:40 and afterload. 0:40 So in total, there are four determinants of cardiac output. So in your vessels, 0:48 your arteries 0:49 and veins, there can be vasoconstriction and vasodilation. This will either 0:53 increase resistance 0:54 or decrease resistance. All in all, this will make up your systemic vascular 0:59 resistance, 1:00 also known as your total peripheral resistance. Thus, your cardiac output and 1:06 your systemic 1:07 vascular resistance can be used to calculate your arterial pressure. And so we 1:15 can say that 1:18 cardiac output multiplied by systemic vascular resistance equals your mean 1:26 arterial pressure. 1:29 On a side note, your mean arterial pressure therefore will affect your after 1:33 load, because 1:33 if it will increase, it will increase your afterload. In your big arteries in 1:39 the body, 1:39 there are special receptors, special pressure receptors called baroreceptors. 1:44 These are 1:44 specifically found in your carotid sinus and your aortic arch. These barorecept 1:50 ors will 1:50 detect an increase or decrease in pressure in the arteries and will relay this 1:56 information 1:57 to the brainstem, to the medulla oblongata, to areas of the medulla called the 2:02 medulla 2:03 vasomotor center and the cardiovascular center. And depending on what the input 2:09 is, the response 2:10 will target different areas of the body. So for example, the response will 2:14 influence the 2:15 systemic vascular resistance, either telling the body to cause vasoconstriction 2:21 or vasodilation. 2:23 The response from the medulla oblongata will also target the contractility of 2:28 the heart. 2:29 So for example, it will tell the heart to increase contractility or decrease 2:35 contractility. 2:36 The medulla vasomotor center will also influence venous return. So how much 2:40 blood is returning 2:41 to the heart and as we know, venous return will affect preload. The 2:47 cardiovascular center 2:49 in the medulla will have a response that will influence your heart rate, either 2:53 decreasing 2:53 your heart rate or increasing your heart rate. It's also important to know that 3:00 your higher 3:01 brain centers also communicate with the medulla vasomotor center and the 3:05 cardiovascular center. 3:07 So for example, in a state of emotion, fear, stress, worry, the higher brain 3:13 centers will 3:14 communicate to the medulla oblongata, telling it to increase your heart rate, 3:20 for example. 3:21 Finally it's important to know that your cardiac output, the amount injected by 3:26 the 3:26 heart in one minute, will also therefore influence your venous return. How much 3:30 blood will return 3:32 to your heart. So I hope this simplified diagram can allow you to understand 3:37 the relationship 3:38 between different things, between the arterial pressure, cardiac output and the 3:43 determinants 3:44 of cardiac output itself and the response from the medulla vasomotor center and 3:49 the 3:49 cardiovascular center. Just to recap, the mean arterial pressure is the cardiac 3:54 output 3:54 multiplied by systemic vascular resistance. But clinically, the mean arterial 3:59 pressure 3:59 is calculated with a different equation, which is diastolic blood pressure plus 4:05 one-third 4:05 of systolic blood pressure minus diastolic blood pressure. What does this mean? 4:11 Let's 4:11 look at a diagram to explain. So here we have the pressure from zero mill 4:17 imeters mercury. 4:19 The diastolic blood pressure, if you imagine we're measuring the pressure 4:23 around the aorta 4:24 during diastole, which is the phase when the ventricles are being filled with 4:29 blood. The 4:30 diastolic blood pressure of an average adult is about 80 millimeters mercury. 4:36 Cystole is 4:37 when the ventricles are contracting, ejecting the blood out of the heart. 4:41 Imagine measuring 4:42 the pressure in the aorta during systole. The average systolic blood pressure 4:48 in an adult 4:48 is about 120 millimeters mercury. And obviously during diastole and systole, 4:54 the pressure fluctuates 4:56 going up in systole and going back down during diastole. The mean arterial 5:02 pressure is about 5:02 one-third of systolic blood pressure minus diastolic blood pressure. And so in 5:08 order 5:09 to calculate this mean arterial pressure, it's essentially calculated the diast 5:13 olic blood 5:14 pressure, which is about 80, and then one-third of systolic blood pressure 5:19 minus diastolic 5:20 blood pressure. I hope this made sense. Thank you for watching.