Pelvic Inflammatory Disease
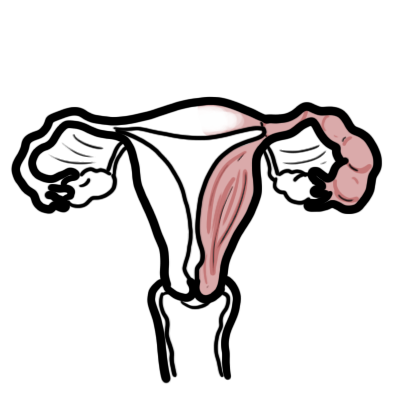

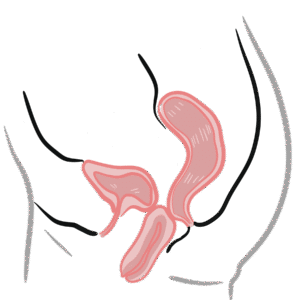
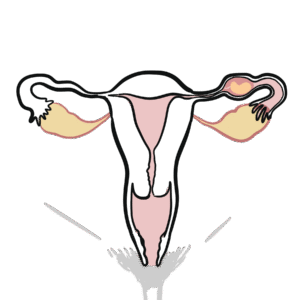
Pelvic inflammatory disease (PID) comprises a spectrum of inflammatory disorders of the upper female genital tract, including any combination of endometritis, salpingitis, tubo-ovarian abscess, and pelvic peritonitis. Causative organisms are either sexually transmitted (such as C trachomatis, N gonorrhoeae, Mycoplasma genitalium) or endogenous vaginal organisms (for example, Bacteroides species) that ascend into the pelvic area from the lower genital tract through the cervix. Pelvic inflammatory disease is a major concern because it can result in longterm reproductive disability, including infertility, ectopic pregnancy, and chronic pelvic pain.
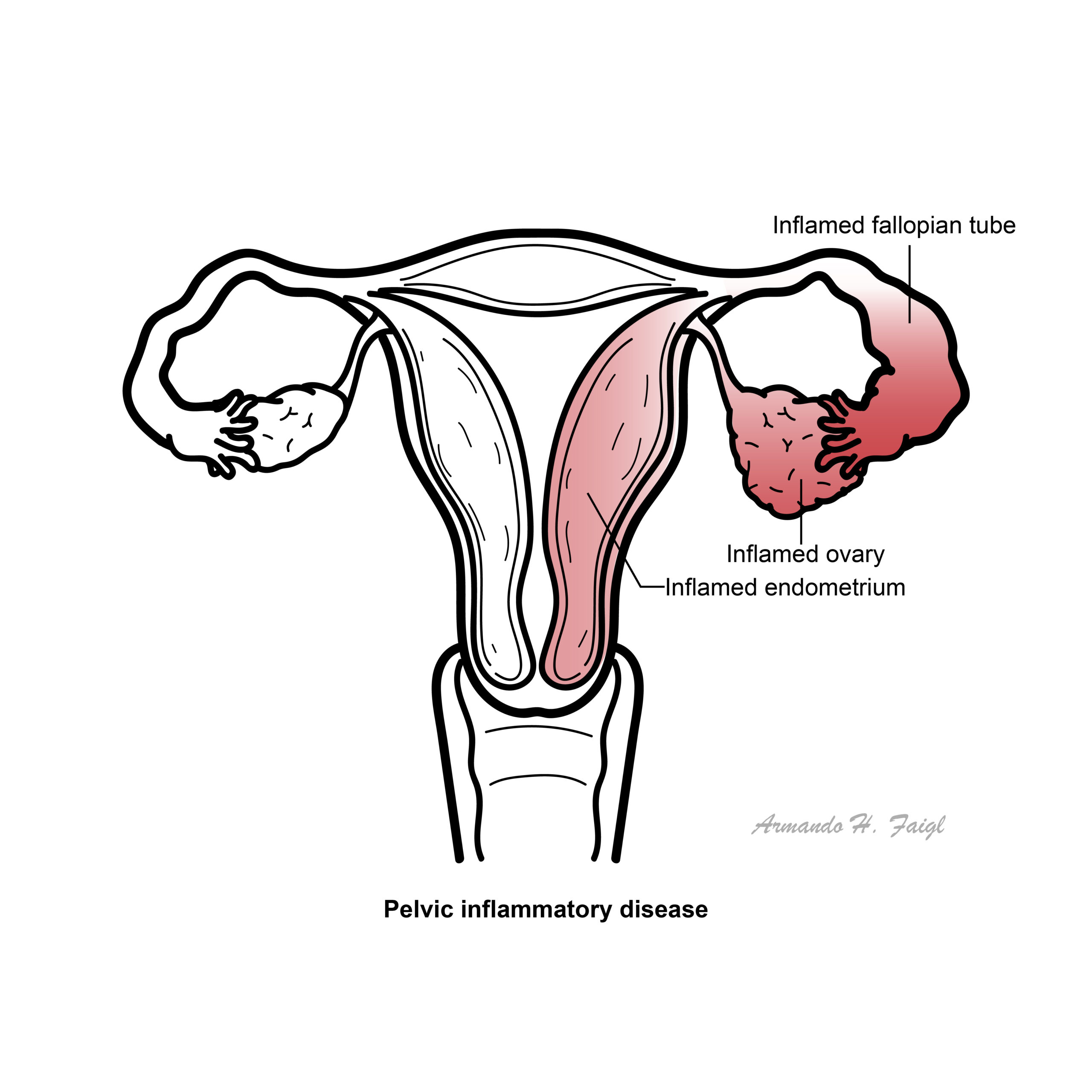
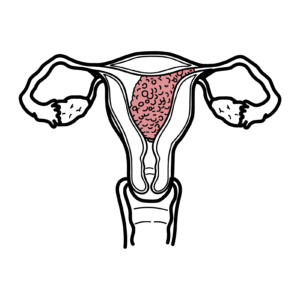
Pelvic Inflammatory Disease: Inflammation and infection of the upper genital tract in women, typically involving the uterus and adnexa.
Mild to moderate PID: Absence of a tubo-ovarian abscess.
Severe PID: Severe systemic symptoms or the presence of a tubo-ovarian abscess.
Vaginal Microbiology
The hydrogen peroxide-producing Lactobacillus species is the most dominant, non-pathogenic organism living in the vagina. The vaginal flora of most normal, healthy women also includes a variety of potentially pathogenic bacteria in low numbers:
Many factors influence the vaginal microflora including:
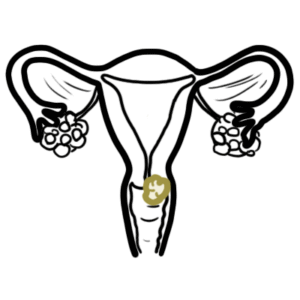
Cervix
The endocervical canal functions as a barrier protecting the normally sterile upper genital tract from the organisms of the dynamic vaginal ecosystem. Endocervical infection with sexually transmitted pathogens can disrupt this barrier.
Pelvic inflammatory disease (PID) is a polymicrobial infection of the upper genital tract that primarily affects young, sexually active women. In most cases, the precise microbial etiology of PID is unknown. When known:
PID can occur after instrumentation of the uterus, such as during D & C for termination of pregnancy or miscarriage, or insertion of an PID.
PID can be caused by polyps, fibroids and neoplasms, which prevent closure of the uterine cavity and allow endogenous organisms to colonise the upper genital tract.
The microorganisms that are implicated in PID are thought to spread in three ways:
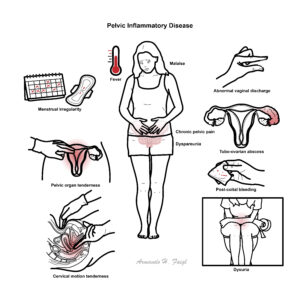
PID is mostly asymptomatic
Acute PID: characterized by the acute onset of lower abdominal or pelvic pain, pelvic organ tenderness, and evidence of inflammation of the genital tract.
Subclinical PID: Subclinical infection of the upper reproductive tract that does not prompt a woman to present to medical care but is severe enough to produce significant sequelae appears to be relatively common.
Chronic PID: An indolent presentation of PID with low-grade fever, weight loss, and abdominal pain has been reported with actinomycosis and tuberculosis.
One or more of the following minimum criteria must be present on pelvic examination to diagnose PID:
The following criteria can improve the specificity of the diagnosis:
The following test results are the most specific criteria for diagnosing PID:
| Condition | Clinical Features |
| Ectopic pregnancy | History of missed menses, positive pregnancy test |
| Ovarian cyst rupture/torsion | Sudden onset of severe pain |
| Endometriosis | Cyclical or chronic pain |
| Cystitis | Urinary frequency and/or dysuria |
| Appendicitis | Pain localized to the right iliac fossa, vomiting |
| Diverticulitis | Bowel symptoms in older women |
| Irritable bowel syndrome | Generalized abdominal pain, constipation, diarrhea |
| Functional pain | Other causes have been excluded |
Empiric antibiotic treatment should be initiated at the time of presentation in patients with symptoms suspicious for PID, even if the diagnosis has not been confirmed. Antibiotics can be any of the following depending on severity and situation:
Remember to test and treat the partner if necessary. Partners should be instructed to abstain from sexual intercourse until they and their sex partners have been adequately treated.
Mild to moderate (outpatient) Oral antibiotics
Severe (Inpatient) IV Antibiotics
Follow up
| Indications for hospitalzation |
| Inability to follow or tolerate an outpatient oral medication regimen |
| Pregnancy |
| No clinical response to oral antimicrobial therapy |
| Severe illness, nausea and vomiting, or high fever |
| Severe illness, nausea and vomiting, or high fever |
| Surgical emergencies (e.g., appendicitis) cannot be excluded |
| Tubo-ovarian abscess |
Pregnant women suspected to have PID are at high risk for maternal morbidity and preterm delivery. These women should be hospitalized and treated with intravenous antibiotics.
Screening for lower genital tract chlamydial infection in younger and high-risk populations is recommended to reduce the incidence of PID. Asymptomatic disease should be treated.
Complications (I-FACE-PID)
Prognosis Patients who have co-existent conditions (HIV infection, pregnancy, IUD, prior PID or tubo-ovarian abscess) require close observation and may require hospitalisation.










Discussion