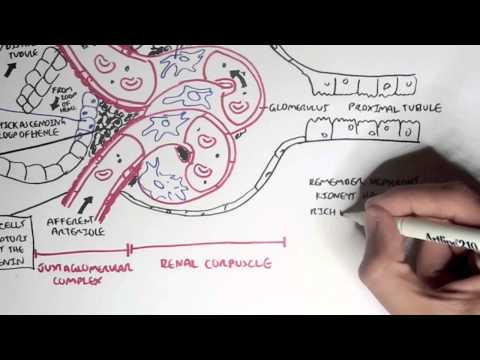
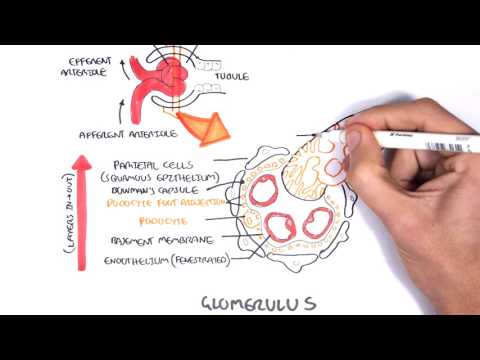
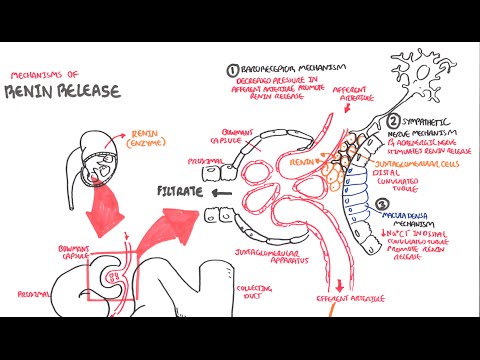
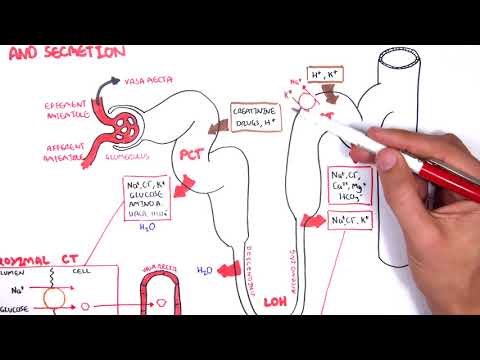
0:00 Armando Hausadoungen, Biology and Medicine videos, please make sure to 0:03 subscribe, join 0:04 the forming group for the latest videos, please visit Facebook, Armando Hausad 0:07 oungen, please 0:08 like and here you can also ask questions, answer questions and post some 0:11 interesting 0:11 things including your hours. 0:12 And you can also change the quality settings to the highest one for 0:15 demographics. 0:16 In this video we're going to continue on from where we last left off, you're on 0:20 production, 0:21 and remember that there are three major renal processes, filtration, reabsor 0:25 ption, secretion, 0:26 and the fourth one we can say is excretion. 0:31 Let's begin looking at urine production by firstly looking at filtration, gl 0:36 omerular filtration, 0:38 which is the first step in urine production. 0:41 So plasma volume entering the Afrin arterial is about 100%, 20% of this is 0:48 filtered into 0:49 the nephron, leaving 80% still in the arterial, in the bloodstream. 0:55 There's 20% which have just been filtered, more than 19% of it will actually be 1:01 reabsorbed 1:02 by the blood. 1:03 And so more than 99% of the plasma return to systemic circulation from entering 1:09 the Afrin 1:10 arterial, meaning that we have less than 1% of the volume of the plasma 1:15 actually excreted. 1:17 I hope this makes sense. 1:21 An important terminology to note is filtration fraction. 1:24 Infraction is the amount of plasma filtered from the glomerular into the neph 1:28 ron, and 1:29 this is 20%. 1:31 Now let's look at how the substances actually get filtered from the glomerular 1:38 into the nephron. 1:40 So here I'm drawing the Afrin arterial and the Afrin arterial coming in, and 1:47 the Afrin 1:48 arterial going out of the bone is capsule. 1:51 Here are the glomerular capillaries, and this is the bone is capsule. 1:55 We have special cells surrounding this area known as mesinglial cells. 1:59 Mesinglial cells contain active, which perform contraction, and so have an 2:05 important role 2:06 in altering blood flow. 2:08 And then we have these other cells surrounding the arterial known as granular 2:12 cells. 2:12 And if you remember there, the cells have secreted the hormone renin. 2:16 And then we have the thick ascending limb, which passes in close contact to the 2:20 head 2:20 of the nephron. 2:21 And this is because they contain special cells known as macular dental cells, 2:25 which are chemoresceptors, 2:28 which help balance ion levels of sodium and chloride passing through. 2:37 And finally, the most important thing we should know is that there are pod 2:41 ocytes in the glomerular 2:43 glomerulus. 2:45 Potocytes are important in the filtration process, which is the first step in 2:49 urine production. 2:51 Potocytes have many feet-like projections. 2:53 Let's have a look at how substances get filtered and how podocytes are 2:57 important in this process, 2:59 by taking a cross-section of this glomerular capillary. 3:03 So here we have the actual capillary. 3:08 And here we have mesinglial cells. 3:12 Let's surround the capillaries with its many feet-like projections, like so. 3:18 Remember inside the capillary we have ions, we have red blood cells, solutes, 3:23 essentially. 3:23 Let's take a closer look at these membranes and how substances get filtered. 3:30 Just a quick look. 3:32 The first membrane is the capillaries endothelial cells, which are fenestrated, 3:36 which means 3:36 that they have gaps, allowing for solutes to move from the capillary into the 3:41 nephron. 3:42 The second layer we have the basement membrane, where solutes can still easily 3:46 pass through. 3:46 The outer layer we have podocytes, feet-like projections of podocytes, the foot 3:54 of the 3:55 podocytes. 3:56 And they are spaced out or they can be very close together, and these, and they 4:02 will have 4:04 also gaps between them, allowing for filtration. 4:08 The endothelial cell, the basement membrane, and the podocyte make up the group 4:12 of membranes 4:13 known as the filtration membrane. 4:16 Now the filtration membrane being that where there is a gap is they make a filt 4:22 ration slip, 4:24 which means that substances can actually get filtered from the capillary into 4:28 the nephron. 4:29 The filtration membrane controls what type of substances moves into the nephron 4:35 . 4:35 They actually do not allow big, big molecules to move through, and they do not 4:42 also allow 4:43 big negatively charged molecules to pass through. 4:46 Why is this? 4:47 Well, let's have a look again at the, here we have the glomerular capillary, 4:53 and we have 4:54 substances within this glomerular capillary. 4:57 We have negatively charged proteins, we have negatively charged ions such as 5:01 chloride, 5:01 we have positively charged ions in our sodium, and also we have a negatively 5:05 charged protein, 5:06 so just albumin. 5:09 Now the podocytes and the basement membrane are actually overall negatively 5:15 charged due 5:17 to proteins and carbohydrates on them known as proteoglycans. 5:23 So because of proteoglycans, podocytes and basement membranes are overall 5:27 negatively charged. 5:29 What does this mean? 5:31 It means that positively charged molecules are absorbed more readily and easily 5:34 than 5:34 negatively charged molecules. 5:37 For example, albumin, which can actually pass through because of its good size, 5:42 doesn't 5:43 pass through because it is negatively charged, and so negative repels negative. 5:49 Sodium can easily pass through because it is positively charged, and so it's 5:52 attractive. 5:53 Chloride can actually pass through because it is very small, and even though it 5:56 's negatively 5:57 charged, it can still pass through. 5:59 However, these big, big negatively charged proteins, they will never pass 6:03 through because 6:04 for one, they are too big to pass through, and second, they are negatively 6:07 charged and 6:07 so repel the negativity of the podocytes and the basement membrane, basically 6:12 the glomerular 6:13 capillary. 6:14 Okay, so we know that substances can move from the glomerular capillary into 6:21 the nephron 6:22 because of these filtration slits, but what causes them to move from the glomer 6:27 ulus into 6:28 the nephron? 6:30 Well, pressure causes them to move from the glomerulus into the nephron, so let 6:33 's look 6:34 at filtration pressure and how it causes these substances to move from the gl 6:38 omerulus into 6:39 the nephron. 6:40 Sorry, I'm saying glomerulus in nephron like 20 times. 6:43 So here of the head of the nephron, the bone is capsule and the glomerulus cap 6:46 illary, after 6:47 an arterial going in and after an arterial going out. 6:50 Let's first of all look at the pressures that favor filtration, which is 6:55 outward movement, 6:57 out of the glomerulus. 6:58 And this pressure, which favors filtration, is known as the glomerular hydrost 7:02 otic hydrostatic 7:03 pressure, abbreviated P for pressure, GH. 7:07 And this is about 60 millimeters mercury, and then we have pressures that 7:15 opposes filtration, 7:17 and this is inward, so substances moving back in to the glomerulus. 7:23 And these pressures are the Bowman's capsule pressure, abbreviated P for 7:28 pressure, GBC, 7:29 and this is about 60 millimeters mercury. 7:31 And then we have another one, which opposes filtration, which is the glomerular 7:35 colloid 7:35 osmotic pressure, P for pressure, GCO. 7:39 And this is about 34 millimeters mercury. 7:44 So what does this all mean? 7:46 Well, the net filtration pressure, NFP, would be the outward pressure, meaning 7:53 the movement 7:54 out of the glomerulus, minus the inward pressure, the movement in to the glomer 7:59 ulus. 8:00 So to calculate the net filtration pressure, it would be pressure of hydro-gl 8:07 omerular hydrostatic 8:08 pressure, minus the Bowman's capsule pressure, minus the glomerular colloid osm 8:13 otic pressure. 8:15 So it's 60, minus 16, minus 34. 8:20 And this gives us 10 millimeters mercury, positive 10 millimeters mercury in 8:25 the right 8:26 in the filtration direction. 8:28 So it means that the net filtration would be 10 millimeters mercury. 8:36 And also remember that this pressure and direction makes it favor filtration. 8:43 This concept to understand is what's called GFR, the glomerular filtration rate 8:48 . 8:48 GFR is the volume of fluid that filters into the Bowman's capsule per unit of 8:54 time. 8:55 And this is, on average, for a human, 125 mils per minute, or 180 liters a day. 9:04 So this is just the amount filtered. 9:05 But remember that less than 1% of the volume is actually excreted. 9:11 So to find GFR, we have to find KF and times it by the net filtration rate. 9:18 We know what the net filtration rate is. 9:20 It's about 10 millimeters mercury, right? 9:22 The KF is a glomerular capillary filtration coefficient. 9:25 And this is calculated or found by measuring the surface area of the glomerular 9:30 capillary, 9:31 available for filtration and also its permeability. 9:35 I'm not going to really talk about the KF, but this is just important to know 9:42 how to calculate 9:44 the glomerular filtration rate. 9:47 So why is it important to know how to calculate GFR? 9:50 Well, if we know that KF times net filtration rate equals GFR, we know that if 9:55 we alter 9:56 the net filtration rate, this will also alter the glomerular filtration rate. 10:02 And so the amount of fluid that gets filtered into the bone is capsules. 10:05 And so this will alter the average glomerular filtration rate. 10:09 If the glomerular filtration rate is increased or decreased, this can tell us 10:15 how the kidney 10:16 is functioning. 10:17 If it's low, it means that there's some problem with the kidney. 10:20 If it's high, there's also some problem with the kidney. 10:23 So it's a good indication of kidney function. 10:27 So we can alter NFR to alter GFR. 10:32 And so NFR, if you remember, the net filtration rate, is equal to the glomer 10:36 ular hydrostatic 10:37 pressure minus the bone is capsule pressure minus the glomerular cholid osmotic 10:42 pressure. 10:43 So we can alter net filtration rate by specifically altering the glomerular 10:48 hydrostatic pressure, 10:50 which is the blood pressure entering the glomerular, the glomerulus inside the 10:56 bone is capsule. 10:57 So if we alter the glomerular hydrostatic pressure, we will alter the net filt 11:01 ration rate, which 11:03 will in turn alter the glomerular filtration rate, and therefore the amount of 11:09 fluid which 11:10 gets filtered from the capillary into the bone is capsule. 11:15 I hope this all makes sense. 11:17 It's important to know. 11:18 So essentially here is the net from the head of the net from the afronautial af 11:21 ronautial 11:22 of the bone is capsule. 11:23 Here is the glomerular hydrostatic pressure, PGH. 11:26 So if we alter this, we can alter the NFR and so the GFR. 11:33 Now the glomerular hydrostatic pressure can be altered by changing the 11:37 resistance in the 11:38 afferent or the efferent arterial. 11:42 What do I mean by this? 11:43 So let's just go back to another simple diagram of the net form and the blood 11:49 blood capillary 11:50 coming in. 11:52 If there is no resistance on the afferent arterial, so it's just normal, this 11:56 would mean that 11:58 the glomerular hydrostatic pressure is also normal, which is about 16 mill 12:02 imeters mercury. 12:03 And therefore if the glomerular hydrostatic pressure is normal, this would mean 12:07 that GFR 12:08 would be normal. 12:10 However, if there is an increased resistance on the afferent arterial coming 12:15 into the bone 12:16 is capsule, this would mean that there would be a decrease in glomerular hydro 12:21 static pressure. 12:22 And therefore a decrease in the glomerular filtration rate. 12:29 Now what if the efferent arterial is just normal, but there is an increased 12:33 resistance 12:34 on the efferent arterial, the arterial coming out of the bone is capsule. 12:39 If there is resistance in the efferent arterial, this would mean that we would 12:42 have an increased 12:43 in hydrostatic pressure within the glomerulus. 12:48 And therefore we would have an increased filtration rate, glomerular filtration 12:55 rate. 12:56 So now let me ask, what would happen if instead of having an increased 13:01 resistance on the afferent 13:03 arterial, we have a decreased resistance in the afferent arterial. 13:07 So the afferent arterial coming into the bone is dilated. 13:11 What would this mean? 13:13 Well this would mean that more blood would be able to rush inside and therefore 13:16 this would 13:17 increase the glomerular hydrostatic pressure and therefore the glomerular filt 13:24 ration rate. 13:25 And from all these diagrams we can see that when whatever happens to the glomer 13:30 ular hydrostatic 13:31 pressure will be the same for the glomerular filtration rate. 13:34 So if the hydrostatic pressure increases, the GFR also increases, if the hydro 13:38 static pressure 13:38 decreases, the GFR also decreases. 13:41 So that concludes this video on glomerular filtration and this video only 13:46 looked at filtration, 13:47 everything to do with filtration. 13:48 The first step in your own production, in the next video we'll look at reabsor 13:52 ption, 13:52 how the filtrate gets reabsorbed back into the blood and that's the second step 13:57 of your 13:57 own production. 13:58 Thank you.