
| Watch Acute Cholecystitis |
Overview
Overview most common complication of gallstones disease. Inflammation of the gallbladder wall associated with abdominal pain, RUQ tenderness, fever, and leukocytosis is the hallmark. Gallstone prevalence: 8% of those over 40years. Up to 90% remain asymptomatic.
Sign and Symptoms
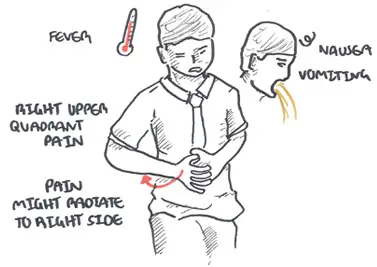
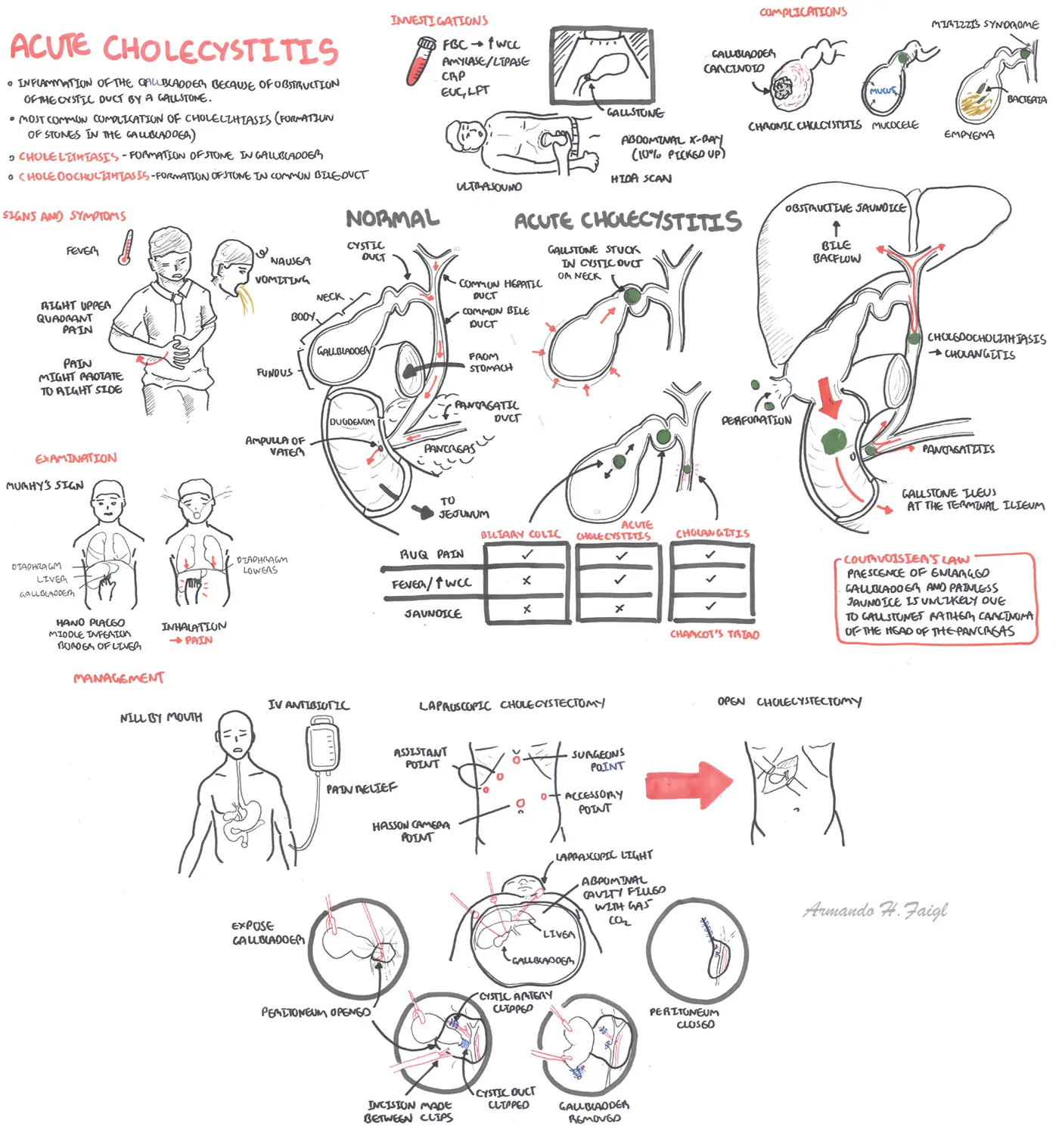
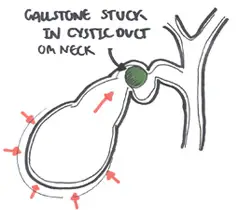
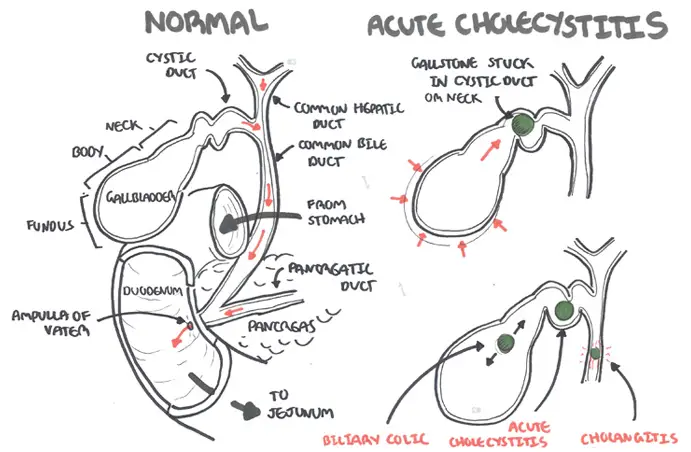
Clinical Presentation Impaction of the neck of gallbladder causes acute cholecystitis which present as severe continous right upper quadrant pain, often radiating to the right flank and back associated with anorexia and pyrexia. Tenderness over gallbladder during inspiration -> Murphy's sign.
| Courvoisier's Law: The presence of jaundice, palpable gallbladder means that the jaundice is unlikely to be due to stones. It is tumour of the head of the pancreas until proven otherwise. |
Examination
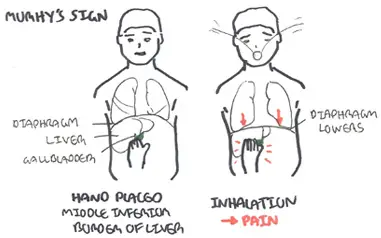
Murphy's Sign classic for acute cholecystitis
Differential Diagnosis
- Appendicitis
- Acute pancreatitis (can be due to gallstones)
- Pyelonephritis
- Hepatic abscess
- Hepatic tumour
- Gonococcal or chylamdial perihepatitis

| Difference between common biliary tree causes of RUQ pain | |||
| Acute Cholecystitis | Biliary Colic | Cholangitis | |
| Overview | Inflammation of the gallbladder due to bile flow obstruction | ||
| Clinical Presentation | Severe RUQ pain, often radiates to the right flank and back associated with anorexia and vomiting. | Intermittent sever epigastric and RUQ pain; usually asssociated with nausea and vomiting. Tenderness over gall bladder during acute episodes. | |
| Management | Cholecystectomy | Conservative | |
| Prognosis | Good | Resolves after few hours | |
| Clinical difference between acute cholecystitis and cancer of the ball bladder and biliary tree | |||
| Acute Cholecystitis | Cholangiocarcinoma | Adenocarcinoma of the gallbladder | |
| Overview | Inflammation of the gallbladder due to bile flow obstruction | Tumour arises in the extrahepatic biliary tree, but may be intrahepatic: usually common bile duct or hepatic duct | Tumour arises from glandular tissue in the gall bladder. Gallstones are found in 70% of cases |
| Clinical Presentation | Severe RUQ pain, often radiates to the right flank and back associated with anorexia and vomiting. | Associated with Ulcerative Colitis and primary sclerosing cholangitis. May present as a gall bladder mass or obstructive jaundice due to local invasion of the common hepatic duct. | |
| Management | Cholecystectomy | Radical excision of bile duct with reconstruction | Radical cholecystectomy |
| Prognosis | Good | Medial survival 9 months | 5 year survival <9% |
Investigation
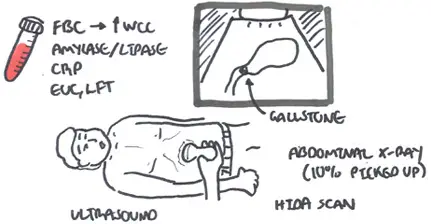
Investigation Check bloods which will show increase WCC. Ultrasound can show a thick-wall, shrunken gall bladder (also seen in chronic), fluid, stones, +/-dilated common bile duct. HIDA can be used if uncertain after ultrasound. Plain abdominal X-ray only reveal 10% of calculi, and it may identify porcelain gallbladder.
| Remember On ultrasound findings suggestive of an ultrasound echogenic focus (dense) and acoustic shadow |
Diagnosis
- History, examination suggestive of acute cholecytitis
- Wall thickening or oedema (ultrasound)
- Sonographic Murphy's sign
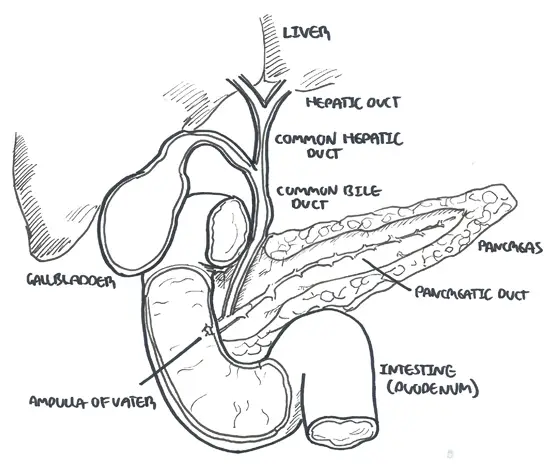
Anatomy and Physiology
Pathology
First few days, the gallbladder is usually distended and contains a stone embedded in the cystic duct. Histologically, range from mild acute inflammation with oedema to necrosis and perforation of the gallbladder wall.
Management
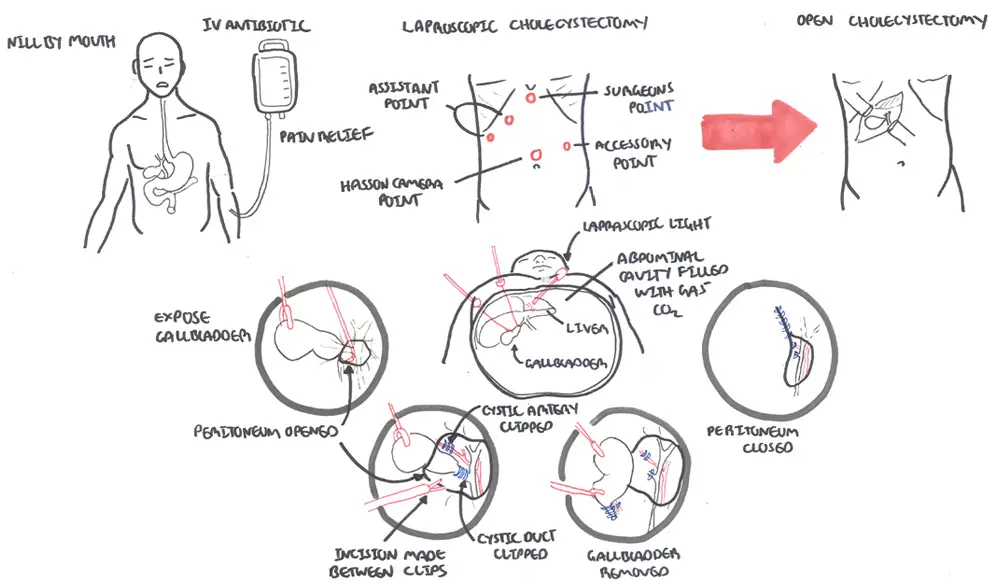
Management Nil by mouth if the patient has a distended abdomen or persistent vomiting, use a nasogastric tube. Provide analgesia and anti-emetic. Oxygen and fluids if needed. Antibiotics (if patient appear toxic or is suspected of gallbladder perforation) and refer to surgeon. Surgical treatment is cholecystectomy.
Laproscopic vs. Open Cholecystectomy In acute cholecystitis, post-operative morbidity, mortality and hospital stay were reduced by laparoscopic cholecystectomy. Moreover pneumonia and wound infection rate were reduced by laproscopic cholecystectomy. Severe haemorrhage and bile leakage rates were not influenced by the technique. Cholecystectomy in acute cholecystitis should be attempted laparoscopically first.
Complications and Prognosis
Common
- Biliary colic +/- obstructive jaundice
- Cholangitis - bile duct infection
Uncommon
- Emphysematous cholecytisis - acute infection of the gallbladder wall caused by gas-forming organisms
- Cholesytoenteric fistula -> gallstone ileus
- Mirizzi's syndrome - gallstone becomes impacted in the cystic duct or neck of the gallbladder causing compression of the common bile duct (CBD) or common hepatic duct, resulting in obstruction and jaundice
- Porcelain gallbladder - calcification of gallbladder wall
- Chronic cholecystitis - repeasted episodes of infection causes thickening and fibrosis of gall bladder
- Carinoma of gallbladder
- Empyema and mucocele - obstructed gallbladder fills with mucus secreted by the gallbladder wall/pus from inflammation.
- Abscess (rare) indicated by swinging fever and pain.
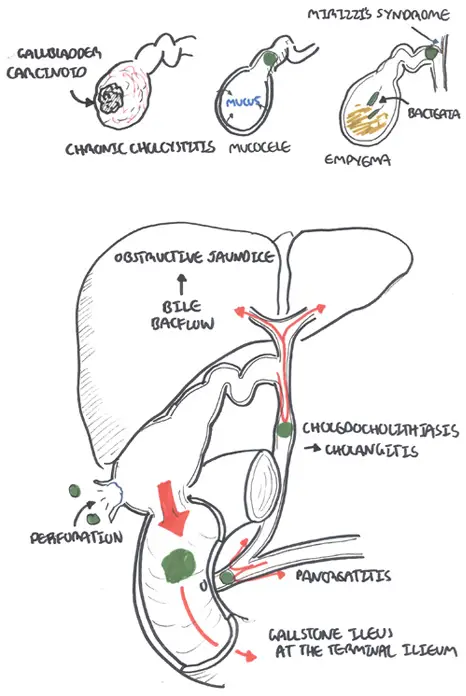
Complications of Acute cholecystitis (biliary colic not included)











