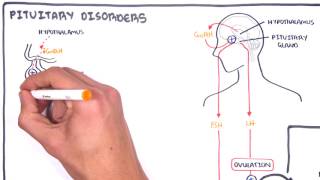
Pelvic organ prolapse is a condition in which pelvic organs abnormally descend or herniate from their normal attachment sites or their normal position in the pelvis to or beyond the vaginal walls. There are varying degrees of prolapse. In the most severe cases, the pelvic organ can prolapse through the genital hiatus. It can be asymptomatic or symptomatic. Very prevalent (~15% of older age women).
Definition
Pelvic organ prolapse: This is a condition in which pelvic organs abnormally descend or herniate from their normal attachment sites or their normal position in the pelvis to or beyond the vaginal walls. There are varying degrees of prolapse. In the most severe cases, the pelvic organ can prolapse through the genital hiatus.
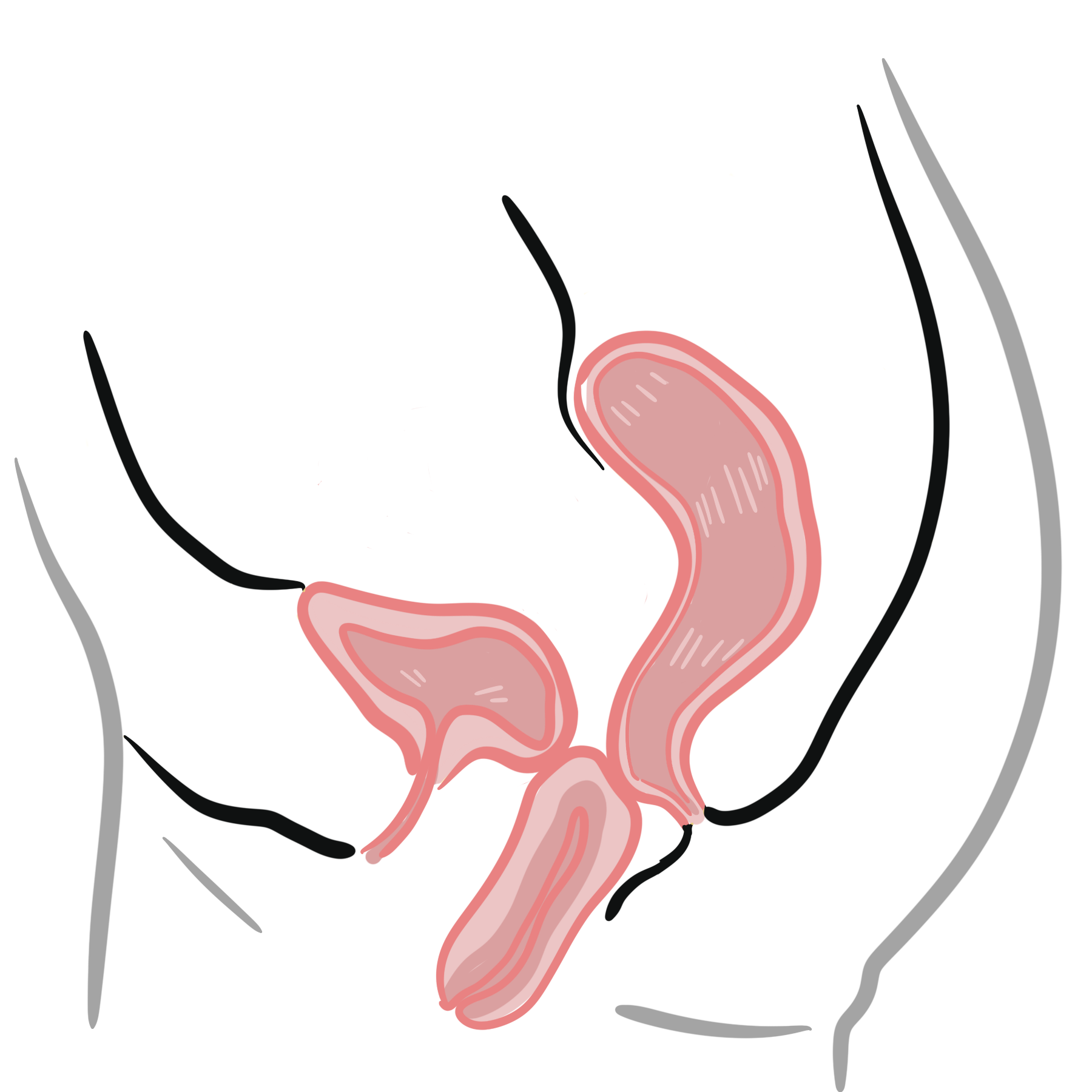
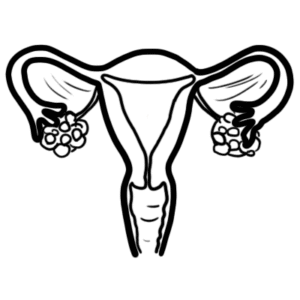
Anatomy
Anatomy – Genital Support (De Lancey – 3 level of support)
Uterosacral and cardinal ligaments – support the uterus and vaginal vault
Bulge or vaginal pressure symptoms This symptom is associated with a prolapse however it does not indicate the stage of prolapse. Anatomically this is defined as a prolapse beyond the hymen
Vaginal or pelvic pressure
Back pain and lower abdominal discomfort
Sensation of a vaginal bulge or something falling out of the vagina
Protrusion of the vagina can also result in chronic discharge and/or bleeding from ulceration
Urinary symptoms Loss of support of the anterior vaginal wall or the vaginal apex can affect the bladder and/or urethral function.
Symptoms of stress urinary incontinence
Defecatory symptoms Affects between 24-52% of women with POP
Faecal urgency, faecal incontinence, obstructive symptoms (e.g. straining, or the need to apply digital pressure to the vagina or perineum to completely evacuate
Haemorrhoids, rectal prolapse may also be present
Sexual function Not associated with decreased sexual desire or with dyspareunia
Some women however avoid sexual activity due to fear of discomfort or embarrassment especially if they develop urinary or fecal incontinence during sexual activity.
Coital difficulty
Menstruating women may also find difficulty inserting tampons
Examination
Pelvic Examination
Speculum with Valsalva maneuver (cough)
Bimanual and rectovaginal examinations help identify any coexisting pelvic abnormalities
+/0 Standing position while she performs the Valsalva maneuver
TYPES OF PROLAPSE
Condition
Feature
Uterine prolapse
Cystocele
Rectocele
Enterocele
Vaginal vault prolapse
Uterine procidentia
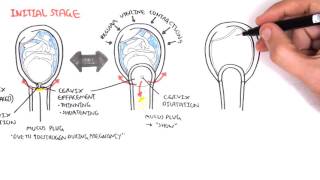
Classification of Pelvic Organ Prolapse
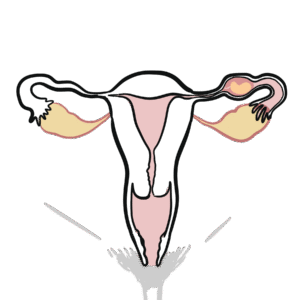
Different types of Pelvic organ prolapse
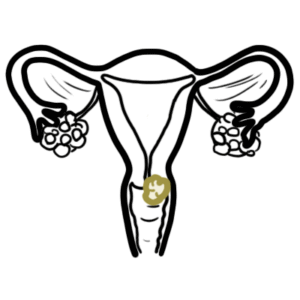
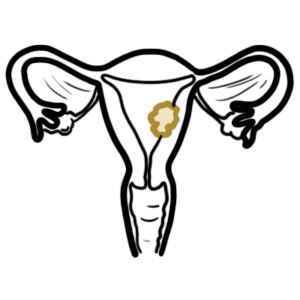
Cystocele – Anterior vaginal wall prolapse – descent of the front wall of the vagina often with the bladder behind
Rectocoele -Posterior vaginal wall prolapse – descent of the posterior vaginal wall often with rectum protruding (bulges forward) into the vagina
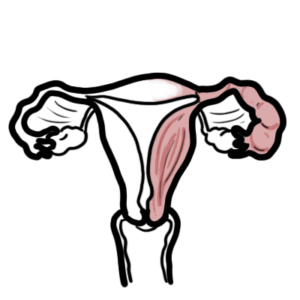
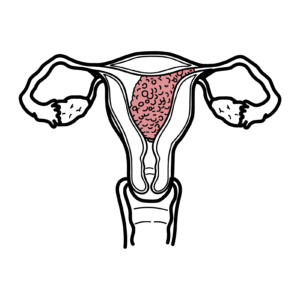
Uterine prolapse – Descent of the uterus
Vault prolapse – Descent of the vaginal vault and may occur in women who have had a hysterectomy. There is frequently small bowel behind a vault prolapse in which it is called an enterocele. This name may also be given to prolapse of the upper part of the posterior vaginal wall i.e. with the uterus still in situ.
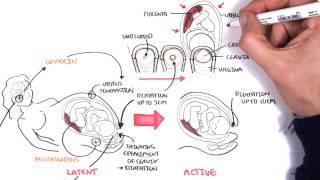
Grades of uterine prolapse
1st degree: Uterine prolapse descents to 1cm above hymen
2nd degree: Uterine prolapse descents from 1cm above to 1cm below hymen
3rd degree: Prolapse further
4th degree: When the uterus is completely outside the vagina (procidentia)
Investigations
Not really needed unless rectal, uterine pathology suspected.
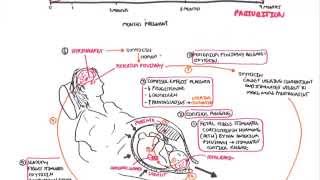
Mechanism of Prolapse
Prevention of prolapse
No effective strategy for primary or secondary prevention
Lifestyle and behavioural factors are appropriate
Not smoking
Maintain healthy body weight
Unclear long term durability. Short-term benefit can be seen with the following.
Elective caesarean delivery
Pelvic floor exercises
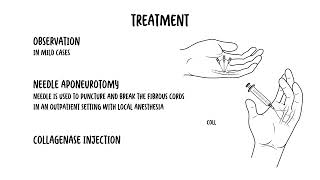
Treatment
The goal of conservative management is to improve symptoms, reduce progression, and avoid or delay surgical treatment.










Discussion