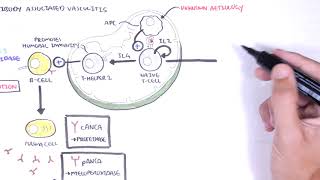
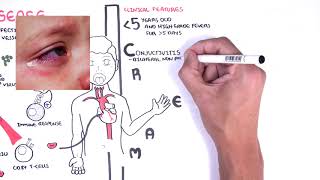
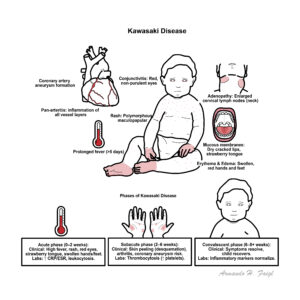
Kawasaki disease is an acute systemic vasculitis affecting small and medium-sized vessels predominantly affecting children under 5 years old. It is the leading cause of acquired heart disease in children in developed countries. Kawasaki is often self-limiting, but 20–25% risk of coronary artery aneurysms if untreated 1.
Definition
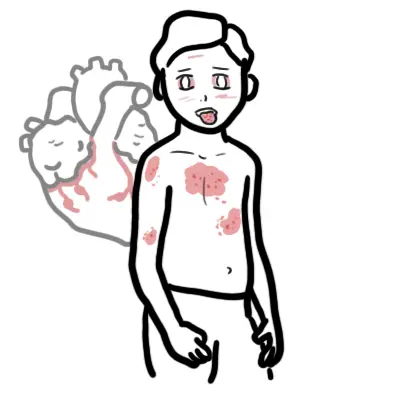
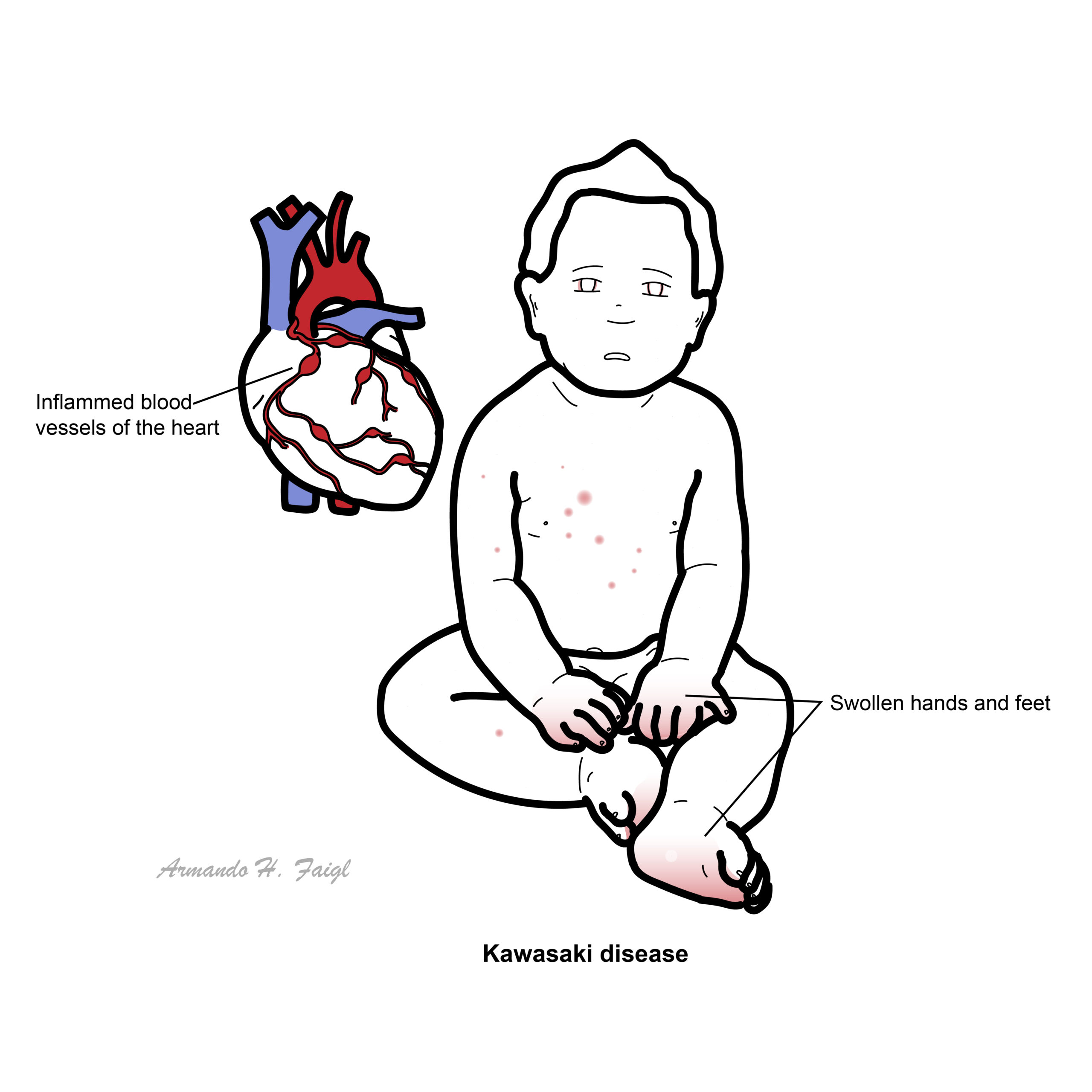
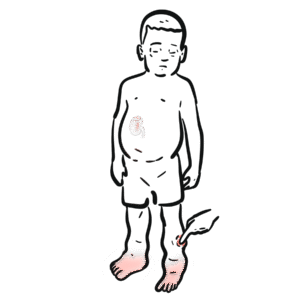
Vasculitis: Inflammation of blood vessel walls, which can lead to vessel wall damage, narrowing, aneurysm formation, or occlusion. In Kawasaki disease, vasculitis predominantly affects medium-sized arteries, especially the coronary arteries. Coronary artery aneurysm: Localised dilation of a section of a coronary artery wall. A feared complication of Kawasaki disease due to inflammation weakening the arterial wall. Can lead to thrombosis, rupture, or myocardial infarction in severe cases. Strawberry tongue: A clinical finding of erythematous, swollen tongue with prominent papillae — a hallmark of mucocutaneous involvement in Kawasaki disease and scarlet fever.
A febrile child with cracked lips, red eyes, and swollen hands may not have an infection — think Kawasaki, not just a viral illness.
Anatomy & Physiology
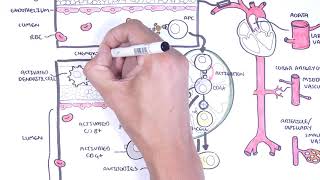
Affects medium-sized muscular arteries, especially coronary arteries. Inflammation involves intima, media, and adventitia of vessels.
Aetiology & Risk Factors
Unknown cause; likely infectious trigger in genetically susceptible host.
Coronary aneurysm regression possible, especially if small.
Long-term cardiac surveillance may be needed.
Coronary aneurysm is the most important complication to remember in Kawasaki Disease.
References
McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement. Circulation. 2017;135(17):e927–e999.
Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study. Circulation. 1996;94(6):1379–1385.
Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals. Pediatrics. 2004;114(6):1708–1733.
Singh S, Agarwal S, Bhattad S, et al. Management of Kawasaki disease. Indian J Pediatr. 2016;83(1):77–84.
















Discussion