

Urinary Incontinence
Overview
Urinary incontinence is an important condition because it causes significant distress. Approximately 15% of the general female adult population have a significant problem with urinary incontinence.
Definition
Urinary incontinence: Defined as the condition in which there is invontary loss of urine, which can be objectively demonstrated and which is a social or hygienic problem.
Stress incontinence: Leaking of small amounts of urine during activities that increase pressure inside the abdomen and push down on the bladder
Overflow (Urge) incontinence: Leaking of small amounts of urine associated with an overdistended, hypotonic bladder in the absence of detrusor contractions. This is often associated wtih diabetes melliurs, spinal cord injuries, or lower motot neuropathies. It may also be caused by urethral oedema following pelvic surgery
Midurethral sling procedures: Operations designed to help women with stress incontinence. Mid-urethral sling procedure installs a U-shaped mesh tape under your urethra to give it support
Anatomy and Physiology
Risk Factors
These risk factors are mainly for stress incontinence
Clinical Manifestation
The incidence of urinary incontinence increases with age
- Frequency
- Nocturia
- Urgency – overactive bladder
- Post-coital continence
- Dysuria
Prolapse with coexist with stress incontinenece in over 50% of cases, and an enquiry about symptoms is essential.
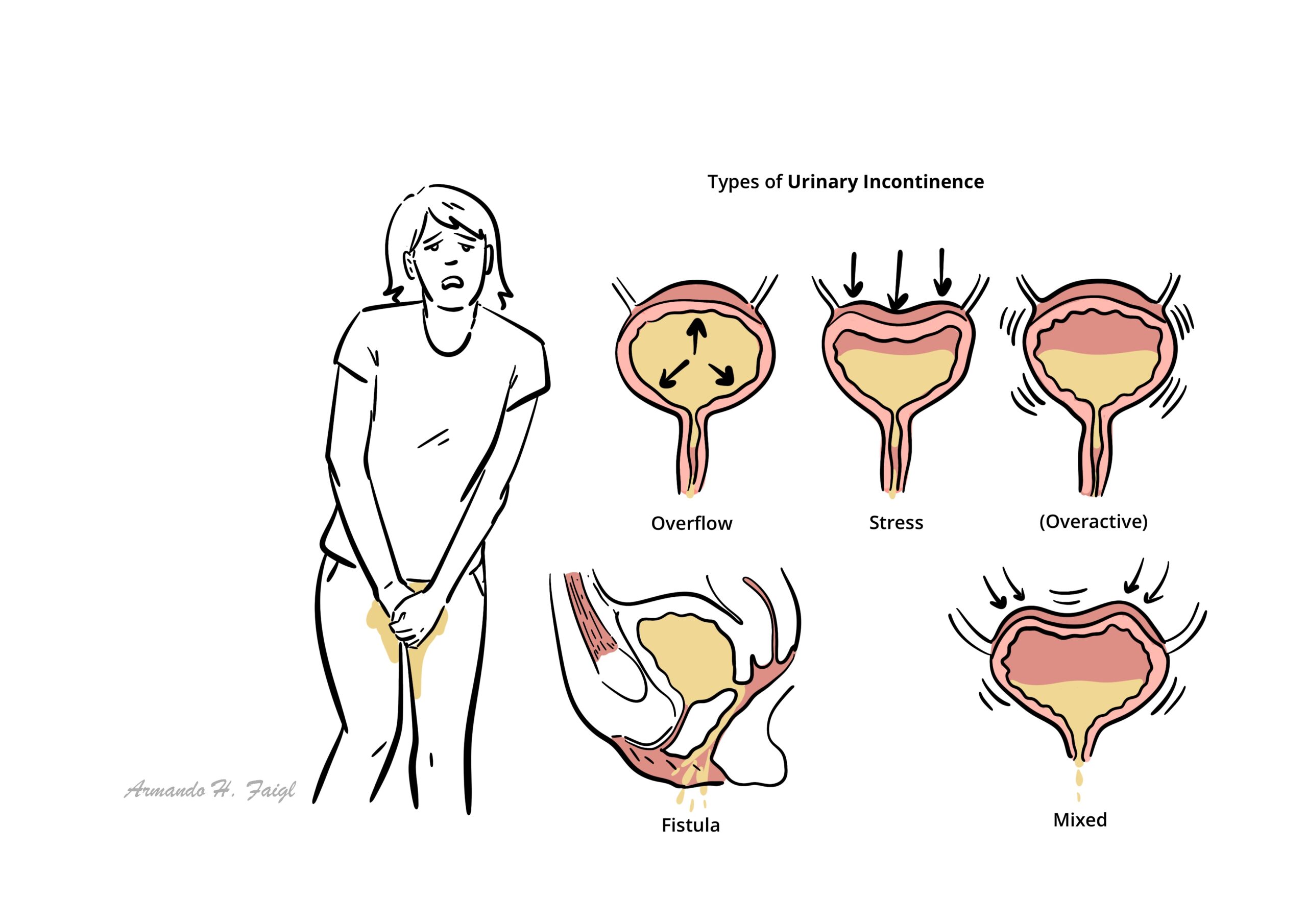
Types of Urinary Incontinence
Types of Urinary Incontinence
- Stress incontinence (most common cause)
- Overactive bladder (Urge Incontinence)
- Mix incontinence
- Retention with overflow
- Fistula
| Types of Urinary Incontinence | Feature |
| Stress incontinence (40%) | Raise in intra-abdominal pressure without detrusor contraction causes urination (i.e coughing, laughing and in severe cases walking) |
| Overactive bladder (25%) | Urgency is the key differentiating factor between overactive bladder and stress incontinence |
| Mixed (30%) | Mixed picture of stress incontinence and overactive bladder |
| Retention with overflow | Often in the eldery caused by neurological problems. The bladder continues to fill until it simply spills over, resulting in leakage |
| Fistula | Communication between two epithelial surfaces, usually a complication of surgery |
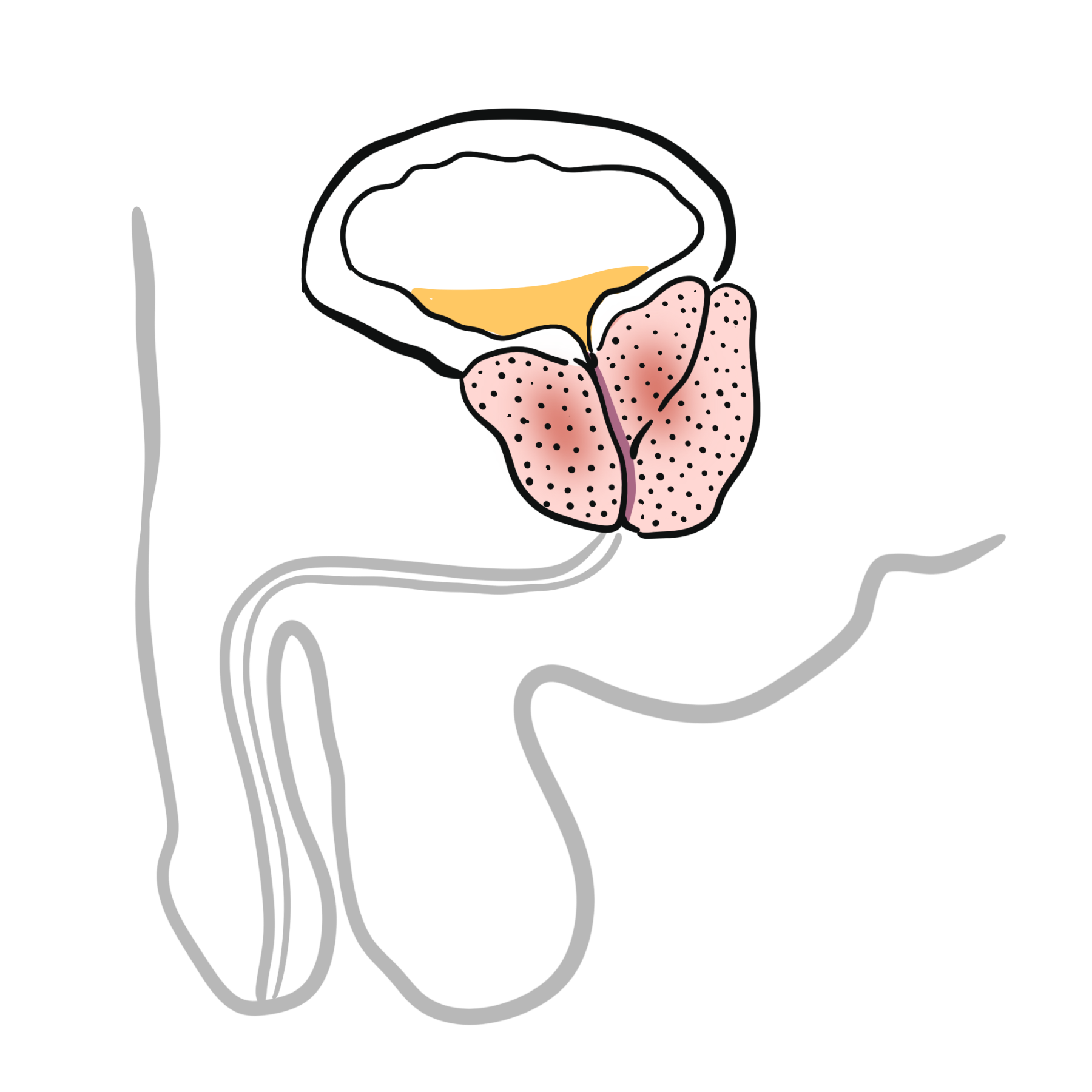
- Benign Prostatic Hyperplasia (men)
- Prostate tumour (men)
- Urinary Tract infections
- Faecal impaction
- Oestrogen deficiency
- Depression
- Restricted mobility
- Drug induced (diuretics)
Investigations
Diagnosis of urinary incontinence may be based on symptoms or urodynamic studies. All women should have a full story and clinical examination.
- Urinalysis – Rule out Urinary tract infections
- Mid Stream Urine Sample – Rule out Urinary tract infections
- Frequency-volume chart
- Ultrasound
- Urodynamic studies
- Cystoscopy – only for assessment of haematuria or recurrent urinary tract infections
| Indication for urodynamic studies |
| Voiding difficulties |
| Neurological disease |
| Failure of conservative management |
| Prior to surgery |
| When surgery has failed |
Treatment
Lifestyle advice is an essential starting point in the management of incontinence.
Conservation Treatment
- Weight loss
- Normalise fluid intake
- Cut down alcohol and restrict caffeine
- Stop smoking
- Avoid carbonated drinks
- Treat chronic constipation and chronic cough
- Bladder retaining
- Physiotherapy – pevic floor muscle training
Medical Treatment – Usually for Stress Incontinence
- Oestrogen – for postmenopausal women
- Anticholinergic – for overactive bladder stress incontinence
- Tricyclic antidepressants – for overactive bladder stress incontinence
Pharmacology
Anticholinergics inhibit the parasympathetic nervous system activity. The parasympathetic Nervous system is responsible for the rest and digest response and urination is one of them. Side effect of inhibiting the parasympathetic nervous system include dry mouth, dizziness, nausea and constipation.
Surgical Treatment for stress urinary incontinence
- Mid-urethral tapes – common for Stress urinary incontinence
Surgical Treatment for Overactive urinary incontinence
- Sacral nerve root stimulation
- Botulinum toxin A infections
- Detrusor myectomy
- Augmentation Cystoplasty
Complications and Prognosis
- Social complications
- Emotions
- Relationships
- Employment
- Sleep
- Exercise and sport
- Travel and holidays
- 85% cure rate post surgery
References
Macgowan, BA., Owen, P., & Thomson, A. (2014). Clinical Obstetrics & Gyaenacology. 3rd ed. Saunders Elsevier. London.





Members only discussions coming soon…