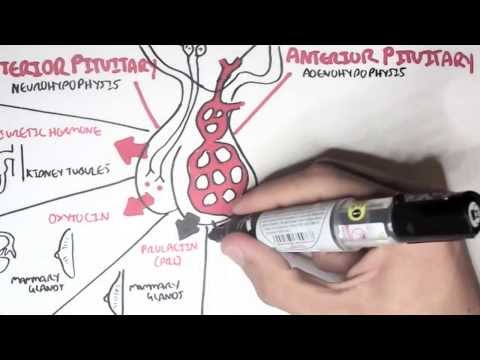
0:00 Diabetes insipidus is associated with inadequate arginine vasopressin, also 0:12 known as antidiuretic 0:14 hormone secretion, or the renal response to antidiuretic hormone. 0:21 So polyureia, dilute urine and increased thirst are characteristic of diabetes 0:28 insipidus. 0:30 The hypothalamus is the region of the brain involved in coordinating the 0:33 physiological 0:34 responses of different organs that together maintain homeostasis. 0:39 The hypothalamus have neurons running towards the posterior pituitary, which 0:44 produce neuropeptides, 0:47 and will release them into circulation. 0:50 These neurons are called magnocellular neurons, and they produce the hormone 0:55 vasopressin, 0:56 also known as antidiuretic hormone, abbreviated ADH. 1:00 It will secrete ADH into circulation via the posterior pituitary. 1:09 Antidiuretic hormone targets the distal part of the nephrons to increase 1:14 channels, which 1:15 will result in water retention. 1:19 The nephrons is made up of the Bowman's capsule, the proximal convoluted tub 1:23 ules, 1:24 the loop of Henley, the distal collecting tubules, and the collecting ducts. 1:30 The afferent arterial carries blood into the nephron, forming the glomerulus. 1:38 The glomerulus will filter blood into the nephron. 1:42 So water and sodium enters, for example. 1:46 Water continues along the nephron tubule, 90% of the water gets reabsorbed back 1:51 into circulation 1:53 at the proximal convoluted tubule via aqua quorum type 1 channels. 2:00 The reabsorption of water back into circulation is actually the reabsorption 2:05 into the vasorecta, 2:07 which is the continuation of the glomerulus and the efferent arterial. 2:13 The vasorecta here in orange functions to secrete and reabsorb things from the 2:18 nephron tubules. 2:22 The remaining 10% of water in the tubule continues through the loop of Henley, 2:27 the distal convoluted 2:28 tubules, and the collecting ducts. 2:31 And it's here at the collecting ducts where the remaining 10% of water can be 2:36 reabsorbed 2:37 in response to ADH. 2:39 Now ADH, also known as vasopressin, increases the expression of aqua quorum 2:46 type 2 channels 2:47 at the collecting ducts, but also at the distal convoluted tubules, causing an 2:54 increase in 2:54 water retention. 2:58 Diabetes insipidus is characterized by polyurea, dilute urine, and increased 3:05 thirst. 3:05 We can group the causes of diabetes insipidus into 4 groups. 3:10 Central diabetes insipidus, primary polydipsia, nephrogenic diabetes insipidus, 3:15 and gestational 3:16 diabetes insipidus. 3:18 All these etiologies present as polyurea. 3:22 And on urine, for example, the urine sample is hypotonic and dilute. 3:28 Tasteless, hence insipidus. 3:32 It's important to rule out other causes of polyurea when doing a urine sample. 3:37 For example, diabetes myelitis is a differential for polyurea. 3:42 In a urine sample, in a patient that has diabetes myelitis, you can look for 3:47 protein 3:48 urea and history of diabetes myelitis. 3:53 Another differential is the intrinsic renal disease. 3:56 And here you can look at renal costs, as well as presence of blood, hematuria. 4:02 Another thing to keep note of is, if it's frequent urination without an 4:08 increase in 4:09 urine volume, suspect urological problems, such as the prostate. 4:15 And these are different to someone that presents with solely diabetes insipidus 4:22 . 4:23 Let's look at these different categories, different causes of diabetes insipid 4:27 us in 4:27 a bit more detail. 4:30 All diabetes insipidus is where you have abnormal synthesis and secretion of 4:36 vasopressin of 4:37 antidiuretic hormone. 4:40 Examples include familial hypothalamic diabetes insipidus. 4:44 This form of diabetes insipidus is due to an inherited mutation of the arginine 4:50 vasopressin 4:51 neurophycin2 gene, inherited in an autosomal dominant manner. 4:57 Tumids, such as craniofarin gioma and pineal gland tumors, which occurs in 5:02 children mainly, 5:04 are another important cause of central diabetes insipidus. 5:10 Trauma and surgery is a very important cause of central diabetes insipidus. 5:16 Surgery and trauma, for example, you can have surgery around the hypothalamic 5:20 area, 5:21 or a pituitary stalk, patients have spasal skull fractures can also have 5:26 diabetes insipidus. 5:30 Primary polydipsia is where you have ingestion of large quantities of water. 5:36 When you drink a lot of water for whatever reason, this can be because of 5:40 uncontrolled 5:41 thirst, the body will tell the brain not to produce antidiuretic hormone as a 5:49 response. 5:49 Another cause of primary polydipsia is if patients have excessive IV fluids. 5:56 This of course causes polyuria. 5:59 The third category for the cause of diabetes insipidus is nephrogenic diabetes 6:06 insipidus, 6:07 which means essentially problems in the response the kidneys have to antidiure 6:13 tic hormone, 6:14 be it a problem in the antidiuretic hormone receptor or the channels itself. 6:21 Specific causes include congenital nephrogenic diabetes insipidus, which is an 6:26 excellent 6:26 mutation of the vasopressin II receptor. 6:29 This means that vasopressin, or ADH, is increased in blood, but has no effect 6:36 on the distal 6:36 convoluted tubules or the collecting duct cells. 6:41 Other causes of nephrogenic diabetes insipidus are acquired. 6:45 Acquired nephrogenic diabetes insipidus include renal disease, such as polycy 6:50 stic keto disease. 6:52 Acquired nephrogenic diabetes insipidus include electrolyte abnormalities, such 6:57 as hypercalcemia 6:58 and hypochlemia. 7:01 Medications such as lithium and the meclocycline can cause acquired nephrogenic 7:06 diabetes insipidus, 7:09 which these medications really damage the nephrons and can result in chronic 7:14 kidney 7:15 disease. 7:16 The last category is gestational diabetes insipidus. 7:20 To understand this, we have to know that antidiuretic hormone is metabolized by 7:26 the liver and also 7:27 by the kidney, and it's excreted by the kidneys. 7:32 Animal diabetes insipidus can cause an increase in the metabolism of ADH, which 7:38 means less 7:39 active ADH, so you have low ADH in the blood. 7:44 And so those are the four categories of diabetes insipidus. 7:49 Remember that in diabetes insipidus, the serum ADH levels can be high or it can 7:54 be low, and 7:55 this will depend on the cause. 8:00 Number one is to perform. 8:02 Because patients present with polyuria, it's good to perform a urine dipstick, 8:07 a urine 8:07 microscopic culture sensitivity, a 24-hour urine output measurement. 8:14 You can use a diary for this, and it's important to rule out other causes of 8:19 polyuria, such 8:20 as diabetes myelitis, as well as some intrinsic renal disease. 8:27 The most important test to probably remember in diabetes insipidus is a 8:32 dehydration test, 8:33 which helps with the diagnosis and differentiation of different types of causes 8:39 for diabetes 8:40 insipidus. 8:43 Dehydration test involves getting the person to not drink for up to 12 hours. 8:48 To understand how the dehydration test works, we need to draw a graph. 8:54 Excess is ours, so patient is dehydrated for up to 12 hours. 9:01 The y-axis, the urine osmolality, really how concentrated the urine is. 9:06 The higher the number, so 1,000, the more concentrated the urine is. 9:12 And as we know, urine is concentrated when we are dehydrated. 9:19 By hours 10 to 12, Desmopressin is given IV. 9:25 Desmopressin is basically the same thing as vasopressin, which is an antidiar 9:29 atic hormone. 9:30 And this is given IV. 9:33 The administration of Desmopressin should make the urine even more concentrated 9:38 because 9:38 the body wants to retain water. 9:42 So you can imagine a normal person undergoing the dehydration test will have an 9:46 increase 9:46 in urine osmolality by 2 to 4 hours. 9:50 And this is because the body is adequately producing vasopressin, and so the 9:55 body will 9:55 retain water and will cause urine to be concentrated. 9:59 By 10 hours when Desmopressin is given, the urine osmolality is really 10:05 unchanged. 10:06 You really have adequate amounts of antidiaratic hormone. 10:11 If a patient has central diabetes incipidus, so no production of ADH, when a 10:18 patient like 10:18 this undergoes a dehydration test, the urine osmolality will be low. 10:23 The urine will be dilute, because ADH is not being produced and the person is 10:28 not retaining 10:29 water, even though they are dehydrated. 10:32 By hour 10, when Desmopressin is given, it will act on the kidneys just like 10:38 vasopressin 10:39 and cause water retention. 10:42 And so you expect to see an increase in urine osmolality. 10:46 You expect to see an increase, basically a concentrated urine. 10:52 The dehydration test is important because it can also help differentiate 10:56 central diabetes 10:57 incipidus with nephrogenic diabetes incipidus. 11:00 In nephrogenic diabetes incipidus, there is antidiaratic hormone present. 11:05 It is being produced, but it doesn't have any effect because of problems in the 11:10 kidneys. 11:11 Nephrogenic diabetes incipidus undergoes a dehydration test. 11:14 The person will have dilute urine, because the body doesn't respond to the ant 11:19 idiaratic 11:20 hormone. 11:22 By hour 10, when Desmopressin is given, the urine osmolality is unchanged. 11:29 Why? 11:30 Well this is because again, the problem is in the kidneys. 11:34 There is sufficient ADH, but it cannot exert its physiological effect. 11:41 Finally, you are able to measure ADH levels anytime really. 12:00 You