

Pregnancy (not a disease)

Overview
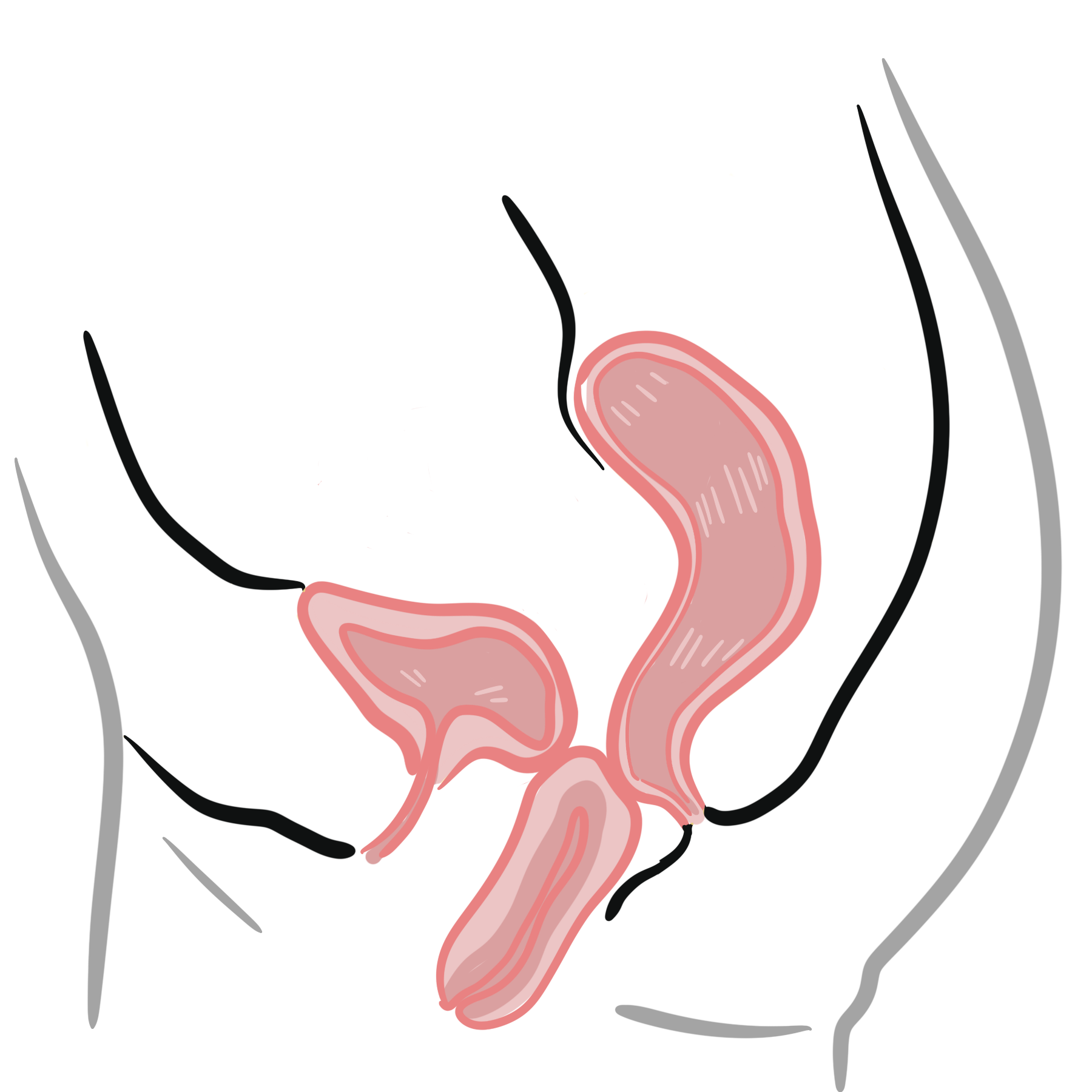
Physiological Changes in Pregnancy
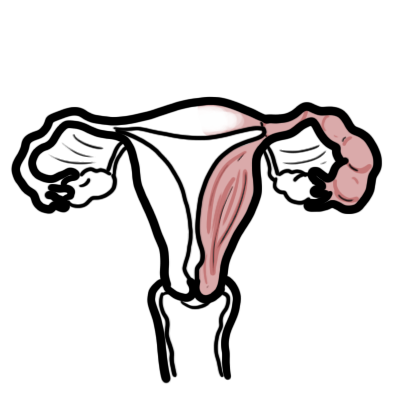
Uterus, Vagina and Breast Physiology changes
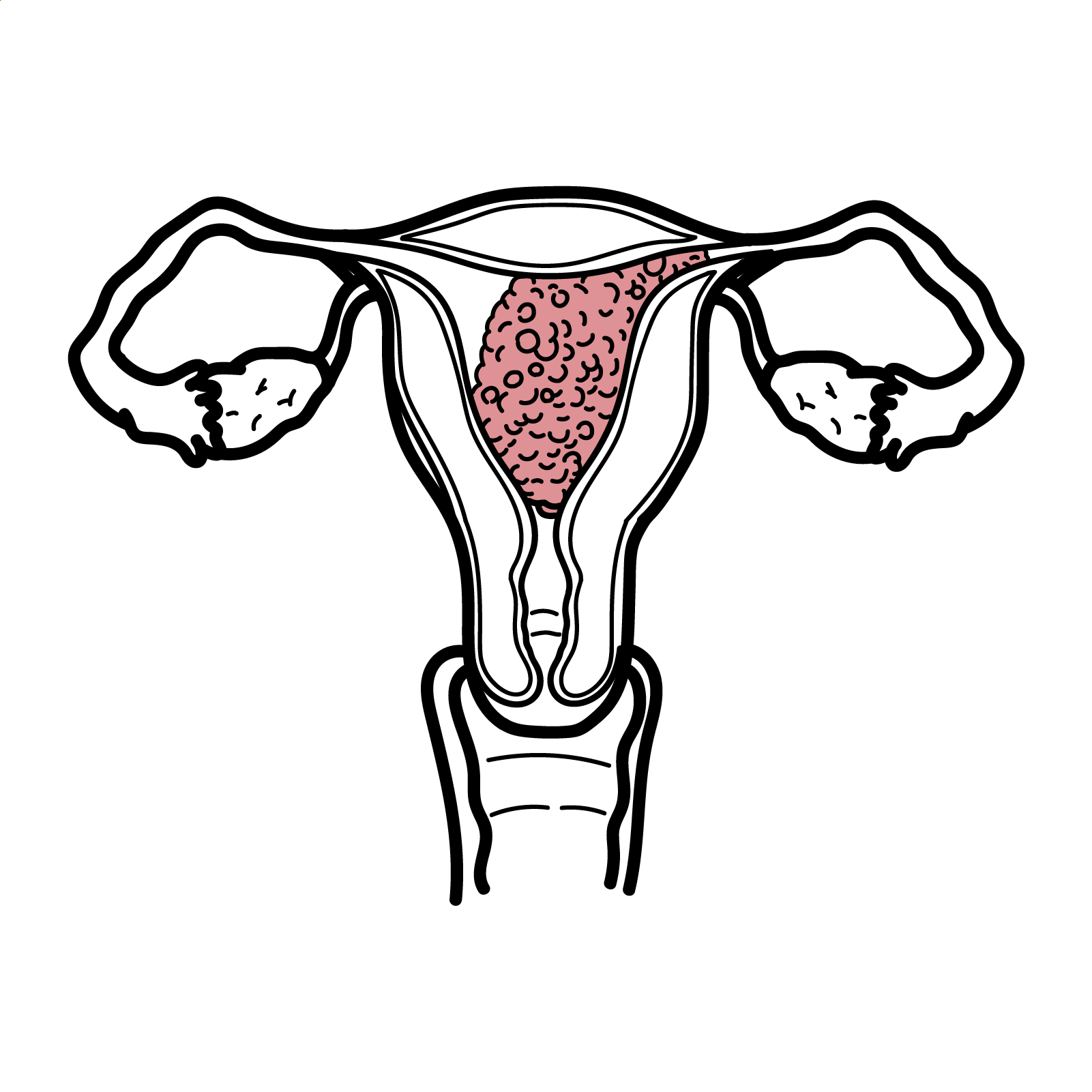
Uterus (Cervix + Isthmus + Body of uterus)
- Muscle hypertrophy til 20weeks then stretching till term.
- Uterine and ovarian arteries undergo hypertrophy
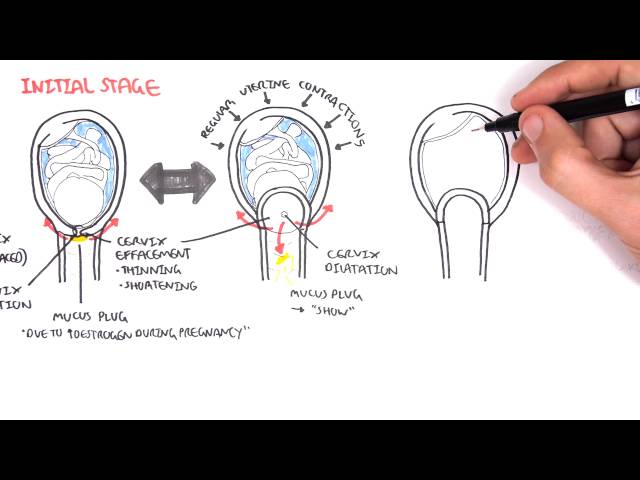
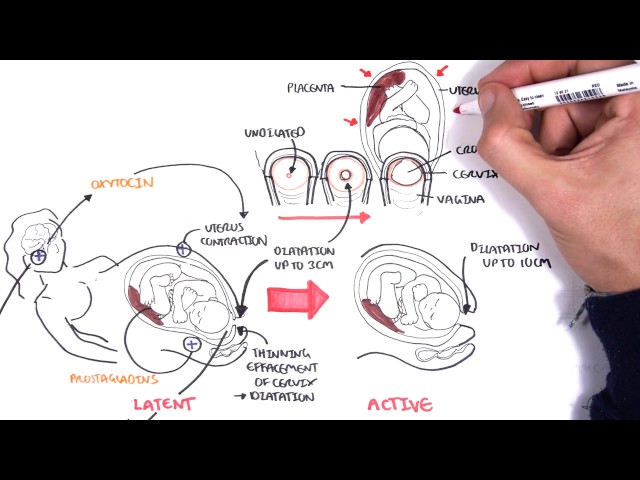
- Cervix
- Reduced collagen → allows dilatation
- Hypertrophy of cervical glands → thick mucus plug
- Uterine body
- ↑size, shape, shape and consitency
- Increases 10-fold
Vagina
- ↑Oestrogen → stimulates glycogen synthesis and deposition in the vagina → lactobacilli proliferation → lactic acid production → decreases pH in the vagina preventing pathogenic bacterial growth
Breast
- ↑Oestrogen → Fat tissue, lactiferous ducts
- ↑Progesterone → Breast lobule
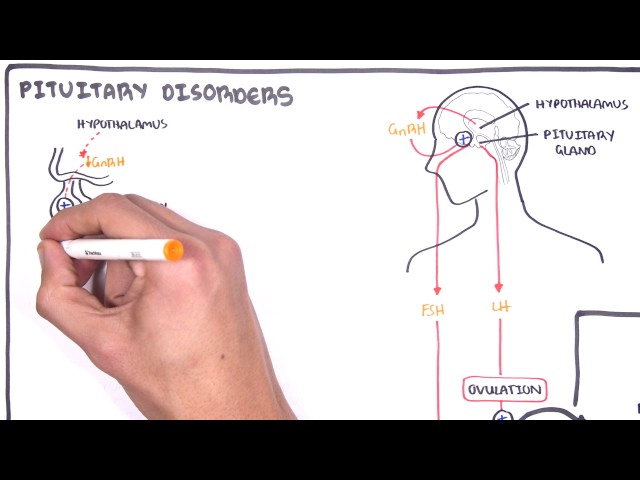
Endocrine Physiology changes
Pituitary Gland
- Enlarges because of ↑anterior lob hormone secretion
- Thyroid gland hypertrophy because of increase demand during pregnancy
That iodine, antithyroid drugs or antibodies associated with thyroid disease can cross the placenta and affect the fetal thyroid function.
Endocrine changes
- ↑Progesterone
- ↑Oestrogen (mainly oestradiol)
- ↑Human placental lactogen
Progesterone
- Causes smooth muscle relaxation
- Reflux
- ↑Tidal volume of lungs
- Prevents preterm labour (because it relaxes the uterus)
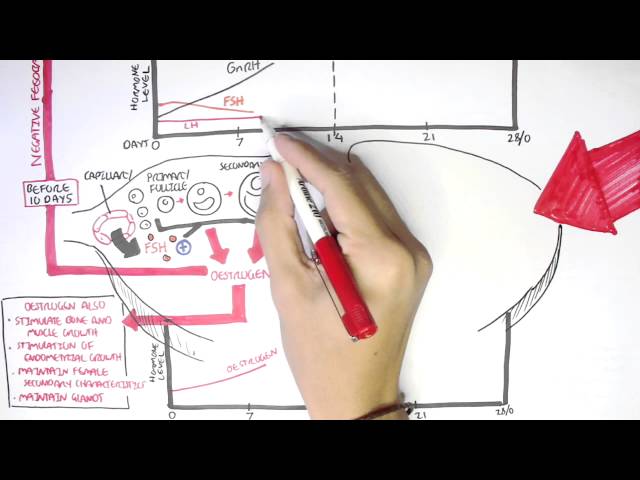
Oestrogen
- Promotes breast and nipple growth
- Increases uterine blood flow, myometrial growth and cervical softening
- Increases sensitivity of myometrial oxytocin receptors
Human placentala lactogen
- Modifies maternal metabolism → ↑energy supply to the featus
- ↑Insulin secretion but ↓insulin peripheral effect, promoting glucose supply to the infant.
Haemtological Physiology Changes
- ↑Plasma volume (~40%) – acute weight gain is commonly due to oedema
- ↑Red cell volume
- ↑WBC – neutophilia specifically
- Slight ↓platelets
- ↑Clotting factors → hypercoagulable state
Respiratory Physiology Changes
- Uterus grows → diaphragm rises → breathing becomes diaphragmatic
- ↑Tidal volume (~40%)
Cardiovascular Physiology Changes
- ↑Cardiac output
- ↑Heart Rate (15bmp) × ↑Stroke Volume (~10%)
- ↓Peripheral resistance
- Blood pressure (most noticeable diastolic) drop by ~15mmhg by mid-term and return back to normal full term.
Urinary Physiology Changes
- ↑Kidney size by 1cm
- ↑ Renal blood flow (~40%) a result of increase cardiac output.
- ↑ Renal blood flow means ↑ GFR
Digestive Physiology changes
- ↑Progestrone → Oesophageal sphincter relaxation → oesophageal reflux
- ↑Progestrone → reduced bowel motility → constipation
- Uterine enlargement → Increase intra-abdominal pressure → worsens reflux + heart burn
Clinical Manifestation
Early Pregnancy
- Amenorrhoea
- Nausea/vomiting – 2/3 of women (morning sickness)
- Breast tenderness and enlargement
- Increased urinary frequency
- Pigmentation of areola
- Dyspnea
- Fatigue
- Light headedness
Late Pregnancy
Hormonal changes
- Nausea and Vomiting
- Gastro-oesophageal reflux (Progesterone)
- Constipation (Progesterone)
- Breast enlargement
- Vaginal discharge
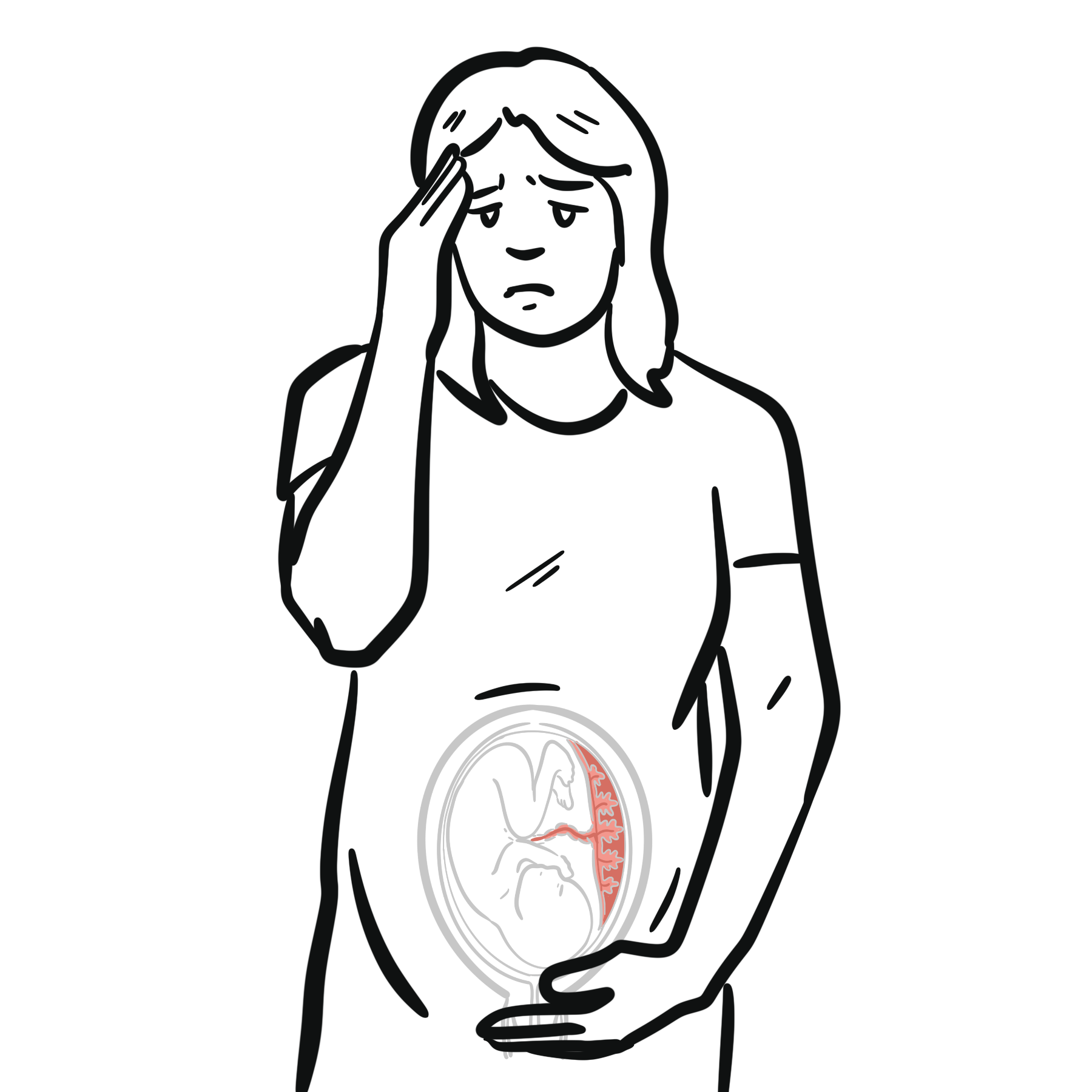
Uterine Enlargement
- Pelvic discomfort
- Backache
- Siatica
- Stress incontinence (3rd trimester)
- Haemorrhoids (3rd trimester)
Other
- Carpal tunnel syndrome
- Polyuria
- Itching and rash
- Headaches
- Dyspnea
- Fatigue
- Insomnia
- Stretch marks
- Calf cramps
- Braxton Hicks contractions
Urinary infections are common in pregnancy. Screen for UTIs!
Diagnosis
Any of the following:
- Beta-hcG in urine or blood (most common)
- Positive ultrasound examination of abdomen
- Fetal cardiac activity on Doppler ultrasound
Supported by:
- Amenorrhoea
- Clinical evidence
ß-hCG is produced by synctiotrophoblast (outside of blastocyst that invades into uterine wall – implantation). ß-hCG prevents degeneration of the corpus luteum (and therefore can continue producing progesterone until placental progesterone can take over at about 6 weeks). B-hcG concentration doubles every 48 hours during first 30-40 days after implantation of a viable, intrauterine pregnancy. After which it slowly rises approximately to 10 weeks then declines until reaching a plateau in 2nd and 3rd trimester.
Causes of slow rise in B-hCG: ectopic pregnancy, miscarriage (not possible to detect off single level – must do multiple tests).
Causes of fall in B-hCG: can be physiological if at 10 weeks but mainly consistent with resolving ectopic, miscarriage.
Antenatal Check
Antenatal check refers to the health care provided to a pregnancy woman throughout pregnancy until labour. Basically a screening program intended to detect complications early, provide health education and implement effective health promotive and preventative interventions.
TIMING (4:2:1)
- 4 weekly till 28 weeks
- 2 weekly from 28 – 34 weeks
- Weekly from 36 till delivery
Normal, uncomplicated pregnancy
- First visit (discussed in detail in next section)
- First ultrasound
Role of ultrasounds: 1st trimester – Determining viable pregnancy versus miscarriage, incomplete miscarriage, molar pregnancy and ectopic pregnancy, Dating scan, Screening (Nuchal fold thickness) and fetal anatomy. 2nd trimester – Fetal anatomy, Fetal measurements, Placental location, Sex of baby (if parents want to know).
| Indications for Ultrasound during pregnancy |
| Routine antenatal check |
| Antepartum Haemorrhage |
| Fundal height is small or large for dates |
| Medical complications of pregnancy – diabetes, Preeclampsia |
| Abnormal foetal presentation |
| Unstable lie at term |
| Placental location if previous scans show LLP |
First Visit to Doctor
Introduction
Confirmation of pregnancy and discussion of models of care
- Establish if planned pregnancy – Affects potential decision for abortion and how the woman will deal/approach pregnancy
- Demographics (age, ethnicity)
- Date of the first day of LMP and thus expected date of delivery
- Use Naegele’s rule, based on 280-day average for each pregnancy i.e. add 9 months and 7 days.
- Importance of dating: antenatal schedule is evidence based and involves tests done at particular times so gestational age should be as accurate as possible.
- Ultrasound sounds also do dating
- Important to keep in mind that Indian or Afro-Caribbean women have shorter gestational times than Caucasians
Naegele’s rule (Nagel’s rule) predicts an estimated due date based on the woman’s last menstrual period.
- Current antenatal history – common symptoms of early pregnancy
- Obstetric history
- Important since previous problems increase the chance of reccurence (e.g. gestational diabetes, pre-eclampsia, miscarriage etc.)
- To establish: previous antenatal/intrapartum/post-partum problems: miscarriages, ectopics, stillbirths, live births, mode of delivery, induction or spontaneous, gestation
- Gravidity and parity (G.P.)
- Breast feeding history – Benefits: better nutrition, GI function, immunological protection, psychological well-being for mother, long term benefits for child
- Gynaecological history
- Date of last pap smear and result
- Previous contraception use
- Gynaecological problems – endometriosis, PID, ovarian cysts, fibroids
- Medical history
- Surgeries
- Medications (inc. vitamins, folate, iodine supplementation)
- Medical conditions (e.g. hyperlipidemia, epilepsy, Graves etc.)
- Allergies
- Immunisation status
- Social History
Smoking is associated with premature birth, placental abruption, miscarriage, low birth weight, still birth, placenta previa.
With Alcohol there is no safe level during pregnancy however 2 standard drinks per day not associated with any adverse pregnancy outcomes. High levels associated with Fetal Alcohol Syndrome.
- Family history – E.g. congenital conditions (heart defects), syndromes (e.g. Down syndrome), cystic fibrosis etc.
Examination
- General Observations
- BMI
- Vital signs
- Cardiovascular exam
- Thyroid exam
- Breast exam
- Abdominal exam
- Vaginal Exam
- Urinalysis
Risk of UTI increases during pregnancy.
Medical Complications During Pregnancy
- Hyperemesis Gravidarum
- Gestational Diabetes
- Thromboembolic disorder
- Anaemia
- Hypertension
- Pre-eclampsia
- PV Bleeding
- Ante-partum haemorrhage
More info Medical Complication During Pregnancy
Unplanned Pregnancy
- Contraception








Members only discussions coming soon…