Psoriasis is a chronic, immune-mediated, inflammatory skin disease with systemic associations, characterized by sharply demarcated erythematous plaques with overlying scale, most commonly plaque psoriasis.[1-4]
It affects about 1% to 3% of the global population, although prevalence varies by geography and ethnicity, and plaque psoriasis accounts for about 80% to 90% of cases.[1,2] Psoriasis is now understood as a multisystem inflammatory disorder rather than a skin-only disease because it is linked to psoriatic arthritis, cardiometabolic disease, obesity, inflammatory bowel disease, and depression.[1,3,4]
Psoriasis: a chronic immune-mediated inflammatory disease affecting skin, nails, and sometimes joints, producing well-demarcated erythematous scaly lesions. Plaque psoriasis (psoriasis vulgaris): the commonest subtype, presenting with symmetric, well-defined red plaques with silvery-white scale. Koebner phenomenon: development of psoriatic lesions at sites of skin trauma, indicating disease activity. Auspitz sign: pinpoint bleeding after removal of scale, classically described in psoriasis, though not required for diagnosis. Psoriatic arthritis (PsA): inflammatory musculoskeletal disease associated with psoriasis, involving peripheral joints, axial skeleton, entheses, or digits.
Psoriasis is a systemic inflammatory disease with skin manifestations, not just “dry skin.”
Anatomy and Physiology
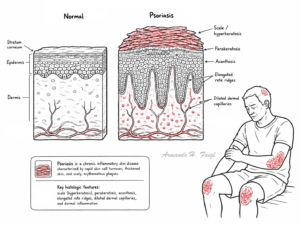
Normal epidermis consists of stratified keratinocytes undergoing orderly maturation from basal layer to cornified layer over roughly 4 weeks; in psoriasis this turnover is dramatically accelerated
The skin immune system includes keratinocytes, dendritic cells, macrophages, neutrophils, and T cells; coordinated cytokine signaling maintains barrier integrity and host defense.
Keratinocytes are not passive bystanders; they both respond to and amplify inflammatory signals by releasing cytokines and chemokines.
Nail unit anatomy is relevant because nail matrix inflammation causes pitting and crumbling, while nail bed inflammation contributes to onycholysis and subungual hyperkeratosis.
Multifactorial disease caused by genetic susceptibility interacting with immune dysregulation and environmental triggers.
Strong genetic contribution, including HLA-C*06:02 and other loci involved in antigen presentation, innate immunity, and NF-kB signaling.
Central immune pathway involves dendritic-cell activation and the IL-23/Th17 axis, with downstream IL-17, TNF-alpha, and other mediators driving keratinocyte hyperproliferation.
Drugs: lithium, beta-blockers, antimalarials, interferons, some NSAIDs; withdrawal of systemic corticosteroids may trigger rebound or pustular flare
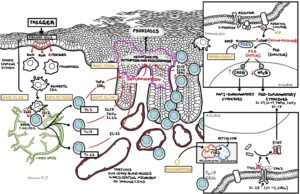
Pathophysiology
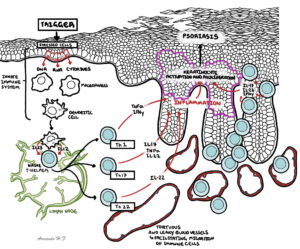
Environmental trigger or trauma activates innate immunity in genetically predisposed skin.
Plasmacytoid and myeloid dendritic cells become activated and release cytokines including interferons, IL-12, and IL-23
IL-23 supports Th17 differentiation and persistence, leading to secretion of IL-17A, IL-17F, IL-22, and other pro-inflammatory mediators.[5,6]
TNF-alpha and IL-17 act on keratinocytes, driving hyperproliferation, abnormal differentiation, angiogenesis, and chemokine release.[3,5,6]
Keratinocytes amplify inflammation further by recruiting neutrophils and additional immune cells, producing a self-sustaining inflammatory loop.
Rapid epidermal turnover leads to retained nuclei in the stratum corneum, thick scale, acanthosis, and characteristic plaques.
This image series is only available to members
This explains why biologics targeting IL-17 and IL-23 can produce very high skin clearance rates in moderate-severe plaque psoriasis.
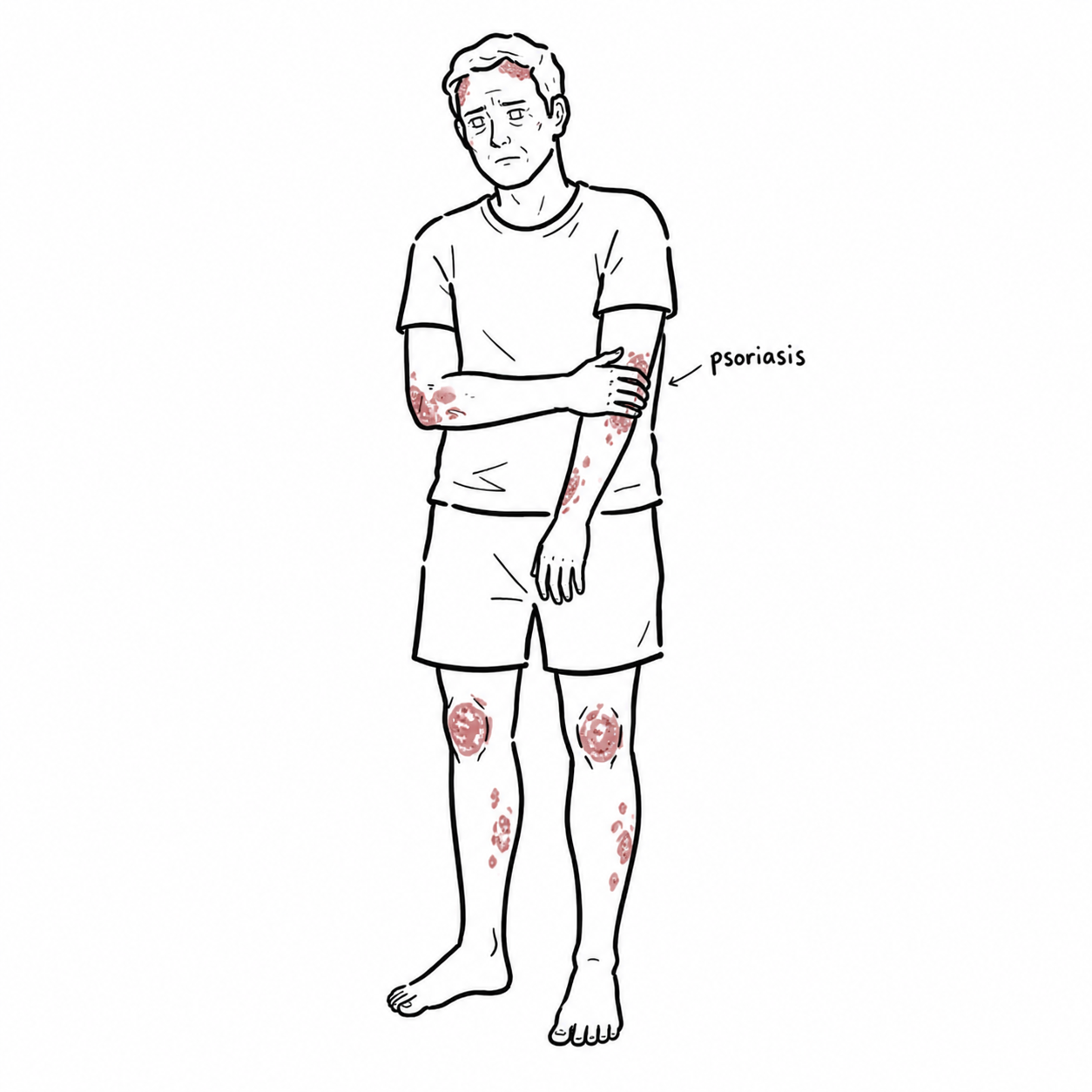
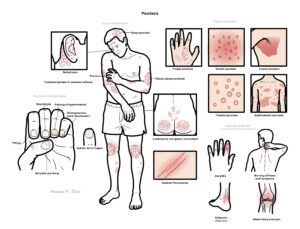
Clinical Manifestation
Well-demarcated erythematous plaques with micaceous or silvery-white scale
Symmetric distribution is typical
Common sites: scalp, elbows, knees, lumbosacral area, umbilicus, gluteal cleft
Pruritus is common; burning, soreness, and fissuring may occur, especially in flexural disease.
Nail dystrophy:
Pitting
Onycholysis
subungual hyperkeratosis
oil-drop/salmon patch discoloration
nail dystrophy.
There are many types of psoriasis and each have their own unique features:
Guttate psoriasis: sudden eruption of small “drop-like” papules, often after streptococcal infection.
Inverse psoriasis: smooth, shiny erythematous plaques in flexures with less scale.
Pustular psoriasis: sterile pustules on erythematous skin; generalized pustular psoriasis can be systemic and severe.
Erythrodermic psoriasis: widespread erythema and scale with risk of systemic instability.
This image series is only available to members
Always inspect scalp, gluteal cleft, umbilicus, nails, and behind ears if psoriasis is suspected. Nail disease should prompt consideration of psoriatic arthritis.
Psoriasis is also associated with the development of psoriatic arthritis an autoimmune disease affecting the enthesis and joints. Features of psoriatic arthritis include: inflammatory joint pain, dactylitis, enthesitis, heel pain, morning stiffness, axial symptoms.
Diagnosis
Diagnostic criteria
No single universal laboratory diagnostic criterion exists for chronic plaque psoriasis; diagnosis is usually clinical, based on characteristic morphology and distribution.
Skin biopsy is reserved for atypical, treatment-resistant, or diagnostically uncertain cases.
Investigation
Clinical skin and nail examination is primary.
Assess severity with BSA, PGA or Physician Global Assessment, symptom burden, and quality-of-life tools such as DLQI; AAD notes PASI is mainly for trials rather than routine day-to-day practice
Skin biopsy
Nail scraping for nail dsytrophy
Screen for psoriatic arthritis by history and targeted joint/enthesis review
In difficult scalp cases, the main distinction is often seborrhoeic dermatitis versus scalp psoriasis versus sebopsoriasis.
Classification
Type
Key features
Plaque psoriasis
Most common; well-demarcated erythematous scaly plaques.
Guttate psoriasis
Numerous small drop-like papules, often post-streptococcal.
Inverse/flexural psoriasis
Shiny erythematous plaques in folds with minimal scale.
Pustular psoriasis
Sterile pustules; localized or generalized.
Erythrodermic psoriasis
Widespread erythema and scaling with systemic risk.
Major psychosocial burden or recurrent unstable flares.
References
Badri T, Kumar P. Plaque Psoriasis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
Psoriasis. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
Man AM, Dinu M, Matei-Man A, et al. Inflammation and Psoriasis: A Comprehensive Review. J Clin Med. 2023;12(22):7149.
American Academy of Dermatology. Psoriasis clinical guideline [Internet]. Rosemont (IL): AAD; updated 2024 [cited 2026 Apr 20].
Potestio L, Camela E, Fabbrocini G, et al. The Role of Interleukin 23/17 Axis in Psoriasis Management. Biomedicines. 2024;12(4):806.
Hawkes JE, Chan TC, Krueger JG. Psoriasis pathogenesis and the development of novel targeted immune therapies. J Allergy Clin Immunol. 2018;140(3):645-53.
Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2023;7(7):CD011535.
National Institute for Health and Care Excellence. Psoriasis: assessment and management. NICE guideline CG153 [Internet]. London: NICE; reviewed 2025 [cited 2026 Apr 20].
Bruno M, Pagnanelli G, Mazzilli S, et al. Topical Management of Plaque Psoriasis—A Review of Topical Therapies, New Developments, and Treatment Strategies. Dermatol Ther (Heidelb). 2023;13:2301-20.
American Academy of Dermatology. Psoriasis treatment: Phototherapy [Internet]. Rosemont (IL): AAD; updated 2024 [cited 2026 Apr 20].
American Academy of Dermatology. Psoriasis treatment: Biologics [Internet]. Rosemont (IL): AAD; updated 2024 [cited 2026 Apr 20].
Aggarwal P, Grewal M, Bhattacharya P, et al. IL-17 and IL-23 Inhibitors Have the Fastest Time to Meaningful Clinical Response in Patients with Plaque Psoriasis. Dermatol Ther (Heidelb). 2024;14:2501-16.
American Academy of Dermatology. Pustular psoriasis: Treatment [Internet]. Rosemont (IL): AAD; updated 2024 [cited 2026 Apr 20].




















Discussion