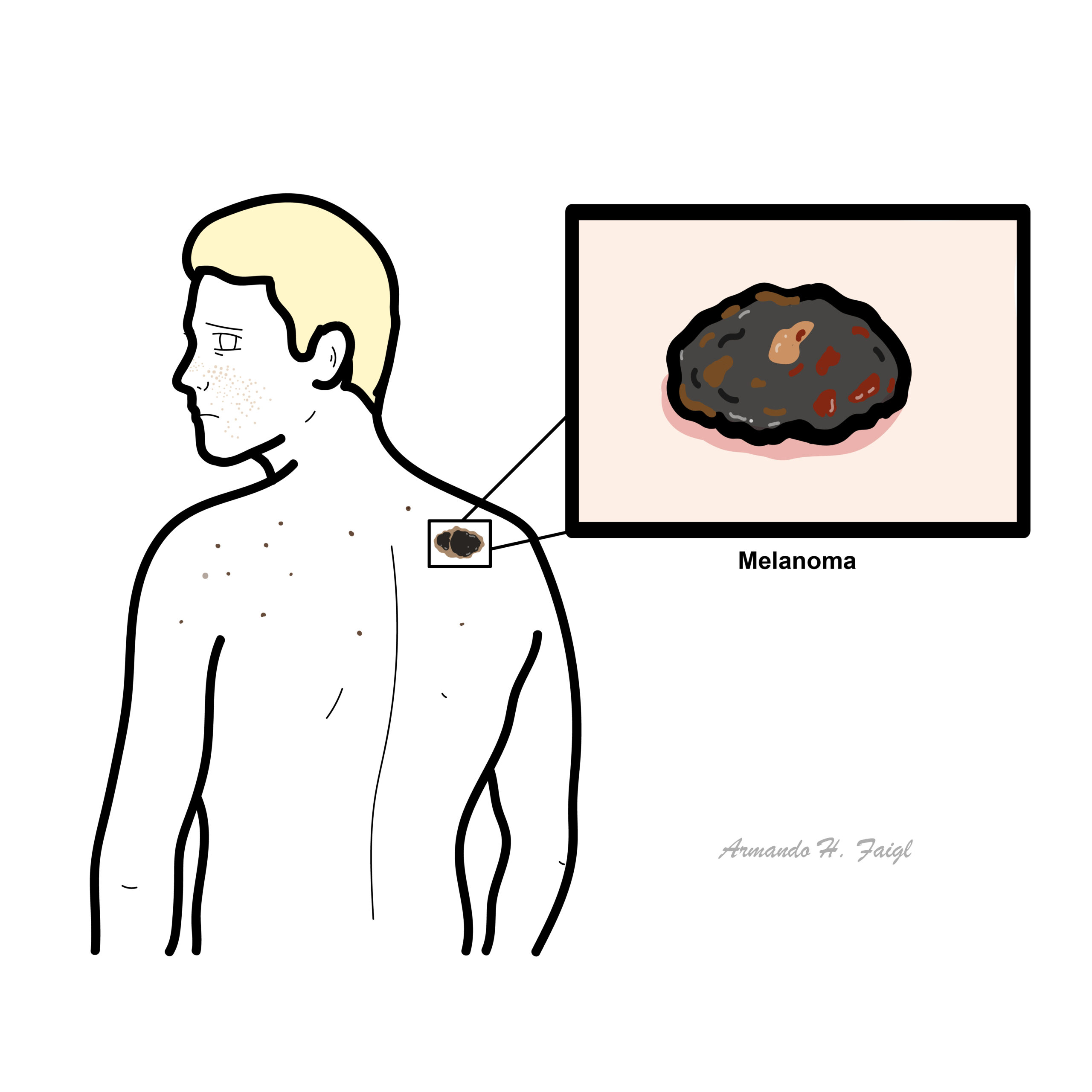
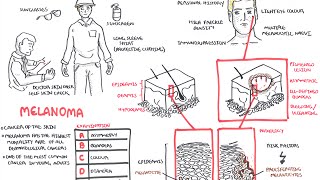
Melanoma

Melanoma accounts for 4 percent of all dermatological cancer. Melanoma has the highest mortality rate of all dermatological cancers, only 14 percent of patients with metastatic melanoma survive for five years. Melanoma is one of the most common cancers in young adults.
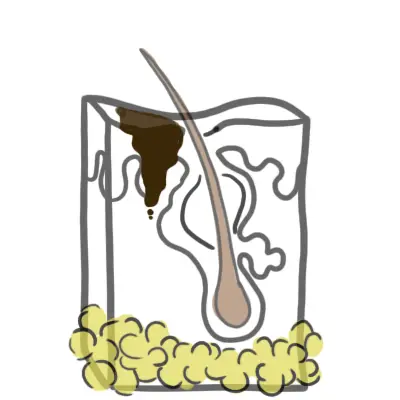
The skin consist of three layers, from superficial to deep:
The epidermal layer are made up mainly of keratinocytes, which are squamous epithelial cells high in keratin (protein). Other cells residing in the epidermis include:
Melanocytes are mature melanin-forming cells found in many parts of the body (eye, ear, hair, heart, bone), but especially in the skin. Through a process called melanogenesis, these cells produce melanin, which is a pigment found in the skin, eye and hair. Vitamin D and UV light stimulate melanocytes to produce melanin.
Mutated BRAF and NRAS genes are most common in superficial spreading and nodular melanoma.
Different types of Melanoma
| Pathological Differences between Benign and Malignant tumours | |
| Malignant | Benign |
| Invasive | Non-Invasive |
| Poorly differentiated | Well Differentiated |
| High mitotic rate | Normal mitotic rate |
| Non-capsulated | Capsulated |
| Usually large growth | Usually small growth |
| Not well circumscribed | Well circumscribed |
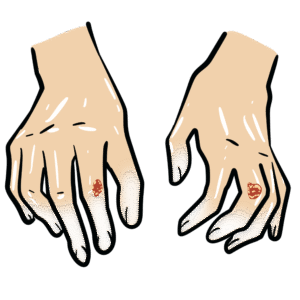
Examination – ABCDE
Blanching. Press down on the lesion for ~3 seconds. Release if pale and refills there is a vascularity involved.
Squamous cell carcinoma is not a good differential because it is not pigmented.
1.4cm depth is dangerous.
| Clark’s Staging – Important histologically | |
| Clark’s Level | Histological characteristic |
| I | Confined to the epidermis “in situ” |
| II | Invasion of the papillary dermis |
| III | Filling of the papillary dermis |
| IV | Invasion of the reticular dermis |
| V | Invasion of the deep, subcutaneous tissue |
| Breslow’s Staging – Important Prognostically | |
| Breslow’s Thickness | Depth of tumour invasion |
| I | ≤0.75mm |
| II | 0.75-1.5mm |
| III | 1.51-2.25mm |
| IV | 2.26-3.0mm |
| V | >3.0mm |
Complication
Metastasis
Treatment adverse effects
Prognosis The most important prognostic indicators are Breslow’s depth of the tumour and lymph node status.
UpToDate
RACGP
Best Practice












Discussion