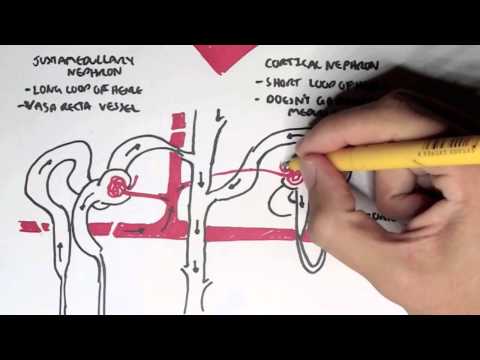
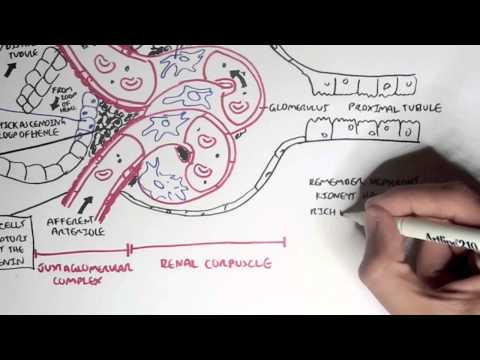
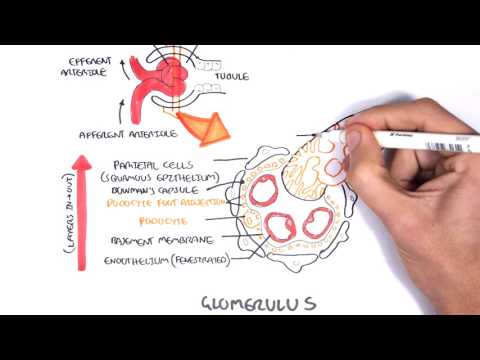
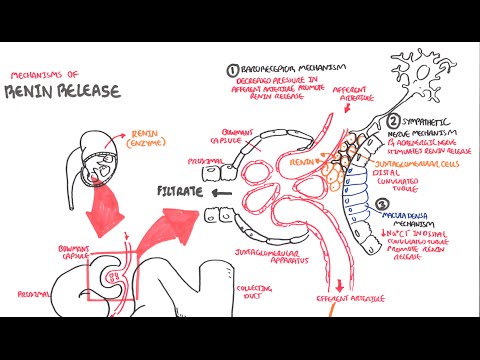
0:00 The kidneys are very important organs. The functional units of the kidneys are 0:11 the nephrons 0:11 and we have millions of these in each kidney. The nephron, the kidneys, are 0:16 important in 0:17 forming urine and there are four main steps in urine formation. These are filt 0:23 ration, 0:23 reabsorption, secretion and excretion. In this video we will focus mainly on re 0:29 absorption 0:30 and secretion. It's important to understand some terminology though. Reabsor 0:36 ption refers 0:37 to the movement of water and solutes from the nephron back into circulation. 0:45 Secretion 0:46 is the movement of solutes and stuff from circulation back into the nephron 0:51 back inside 0:52 the nephron tubule. So let's just recap some anatomy first. 0:57 Here you have the nephron. The afferent arterial brings in blood, brings in 1:02 plasma to the head 1:03 of the nephron where the vessels here will form what's called the glomerulus. 1:08 The vessels 1:08 will then exit the head of the nephron via the efferent arterial. The efferent 1:15 arterial 1:15 will then form the vasorectum which are basically capillaries which will follow 1:20 the tube of 1:21 the nephron. The vasorecta allow for reabsorption of things back into 1:27 circulation while at the 1:28 same time allow for secretion of things from the circulation back inside the ne 1:34 phron tubule. 1:37 Now the tubule of the nephron has a few sections. After the head of the nephron 1:41 , called the 1:42 bermans capsule, you have the proximal convoluted tubules, the loop of Henley, 1:47 the distal convoluted 1:48 tubules and then the collecting duct. These different segments or sections of 1:53 the nephron 1:54 are responsible for the reabsorption of different electrolytes and substances 1:58 as well as water. 2:00 But also these different segments of the nephron may absorb the same things but 2:05 in varying 2:06 amounts. So let's focus on the reabsorption of things first, beginning with the 2:12 proximal 2:12 convoluted tubules. Here you get reabsorption of sodium, chloride, potassium, 2:20 glucose, amino 2:21 acids which are the protein building units, urea and bicarbonate as well as 2:27 water of course. 2:30 In the descending limb of the loop of Henley, water reabsorption takes place. 2:36 In the ascending 2:37 limb of the loop of Henley, so the going up part, sodium, chloride and 2:42 potassium reabsorption 2:43 occurs. The loop of Henley here has a descending limb and is ascending limb as 2:51 we talked about. 2:52 The distal convoluted tubules are responsible for the reabsorption of sodium, 2:57 chloride, 2:58 potassium, calcium, magnesium and bicarbonate. The collecting duct here is 3:05 responsible for 3:05 the reabsorption of sodium, chloride, urea and water. Now different segments of 3:12 the nephrons 3:12 also allow for the secretion of things back inside the tubule from the 3:17 circulation, specifically 3:19 from the vasorecta. Now the proximal convoluted tubule allow for the secretion 3:24 of creatinine, 3:25 certain drugs as well as hydrogen ions which are, if you remember, these guys 3:30 are the acidic 3:31 compounds. And the distal convoluted tubule allow for the secretion of hydrogen 3:36 ions 3:36 as well as potassium. In the distal convoluted tubule there's actually an 3:42 important transporter 3:43 which is actually responsible for the exchange of sodium and potassium and this 3:47 is how the 3:48 potassium enters the tubule of the nephron. And this transport is also a site 3:54 where diuretics 3:55 have an effect. Important things to take note here is that sodium and water 4:00 play a key role 4:01 in regulating our blood pressure. Bicarbonate and hydrogen ions play a key role 4:10 in acid 4:11 base balance so maintaining the pH of our body. So let us now focus on each 4:18 segment or 4:19 each section of the nephron and look into it in a bit more detail, firstly 4:24 focusing on 4:25 the reabsorption of things that occur in this area. So let's look at what 4:30 happens in 4:30 the proximal convoluted tubule and the ascending limb of the loop of Henley. 4:36 The lumen here 4:37 refers to the tubule of the nephron, so inside the nephron tube. And the cells 4:42 here refer 4:43 to the cells which line up the tube of the nephron. And here is the vasorecta 4:48 which is 4:48 a circulation. In the proximal convoluted tubule, sodium get reabsorbed 4:55 together with glucose 4:56 or amino acids. The glucose or amino acid will then get reabsorbed back into 5:02 circulation. 5:04 There is another transporter which uses an exchanger, a sodium for hydrogen 5:10 exchange. 5:11 The sodium is reabsorbed inside the cell and then is exchanged with potassium 5:17 via the sodium 5:18 potassium ATPase pump. The sodium potassium ATPase pump is very important to 5:25 remember 5:26 and it is situated usually on the basal aspect of the cell, so closer towards 5:33 circulation. 5:35 The proximal convoluted tubule is important in regulating acid base balance. It 5:40 is a site 5:40 where hydrogen can be secreted as you can see here, but also it is a site where 5:46 bicarbonate 5:47 can be reabsorbed. What happens is a chemical reaction takes place. Hydrogen 5:54 ions inside 5:55 the lumen of the nephron reacts with bicarbonate ions to form carbonic acid, H2 6:02 CO3. Through 6:03 the enzyme carbonic anhydrase or CA, carbonic acid gets converted to water, H2O 6:11 and carbon 6:12 dioxide CO2. Carbon dioxide is a gas which can diffuse back into the cell. 6:18 Water is also 6:19 present inside the cell and so carbon dioxide can diffuse back into circulation 6:24 because it 6:24 is a gas. Further, within the cell, the same reaction can take place with the 6:29 same enzyme 6:29 carbonic anhydrase, which makes carbonic acid again. Carbonic acid can then 6:35 become hydrogen 6:36 ions and bicarbonate and the cycle can continue. That is why when you have an 6:40 increase in carbon 6:42 dioxide levels, you are more acidic because there is a shift for more hydrogen 6:48 ion production 6:49 and hence more acidity. The hydrogen here can also come from circulation. The b 6:57 icarbonate 6:57 can be reabsorbed into circulation to increase the pH of blood to make it more 7:02 alkali if 7:02 it has to. It does this with a symptoma, a type of transporter which brings 7:08 back into 7:09 circulation bicarbonate and sodium. By carbonate reabsorption in the proximal 7:15 convoluted 7:15 tubule is sodium dependent. It is important to note that other electrolytes are 7:22 also 7:23 reabsorbed in the proximal convoluted tubule which I have not actually drawn, 7:26 and these 7:27 include calcium ions, for example, and majority of calcium is reabsorbed here. 7:35 The ascending 7:36 loop of Henley, not the descending loop of Henley, is a site where electrolytes 7:40 are also 7:41 reabsorbed. There is a trisymptomer, a transporter which brings in one 7:46 potassium, two chloride 7:48 and one sodium, back inside the cell. The potassium and chloride then go 7:54 through another 7:54 symptom which carries it back into circulation. While the sodium gets exchanged 8:00 for potassium 8:02 through again the sodium-potassium ATPase. As you can see, this sort of 8:06 repetition with 8:07 the sodium-potassium ATPase on the basal surface of the cell. In order to note 8:12 here on the 8:13 apical surface on the top of the cells of the loop of Henley, there are passive 8:17 channels 8:17 which allow sodium to enter the cell from the lumen and also potassium to enter 8:22 the lumen 8:23 from the cell. Let us now focus on what happens in more detail at the distal 8:29 convoluted tubule 8:31 as well as the collecting duct. I wrote here distal convoluted tubule and 8:35 collecting duct 8:36 because these parts of the nephrons share some similar functions as well. Again 8:42 , you 8:43 have the lumen of the nephron tubule and the cells which line up the tubule and 8:46 here is 8:47 the vasorecto, which is a circulation essentially. In the distal convoluted tub 8:52 ule, sodium and 8:53 chloride get reabsorbed via a symptom. The chloride has its own channel from 8:59 here back 9:00 into circulation. While sodium actually gets exchanged for potassium via again 9:06 the sodium-potassium 9:07 ATPase on the basal surface of the cell. The potassium can passively go through 9:12 into the 9:13 lumen of the nephron from the cell. Magnesium and calcium reabsorption is 9:22 stored to occur 9:22 via para-cellular roots meaning in between the cells, in between the tight jun 9:28 ctions and 9:28 is stored to occur via diffusion. Now towards the collecting duct there are 9:33 important processes 9:35 which take place and it is here in particular where the last bit of reabsor 9:39 ption and secretion 9:40 takes place before the final urine product is produced. From the lumen of the 9:47 nephron 9:48 sodium is reabsorbed in exchange for hydrogen ions and the reabsorption of 9:52 sodium into circulation 9:54 from inside the cell relies on hydrogen exchange. So now you have sodium in 10:00 circulation and 10:01 you have hydrogen in the lumen. Whenever you have hydrogen in the lumen you 10:05 know acid-base 10:05 balance stuff occurs depending on the pH of the blood. The acid-base regulation 10:10 allows 10:11 hydrogen to interact with bicarbonate ions to become carbonic acid then again 10:17 to carbon 10:17 dioxide and water. The carbon dioxide can diffuse easily inside the cell in and 10:23 out because 10:23 it's a gas. Within the cell however carbon dioxide can react with water again 10:28 and the 10:29 reverse reaction can take place. Water and carbon dioxide become carbonic acid 10:34 and then 10:34 again to bicarbonate and hydrogen ions. Bicarbonate reabsorption into 10:40 circulation uses an exchanger, 10:43 a bicarbonate chloride exchanger and so the big difference to the reabsorption 10:48 of bicarbonate 10:49 here is that it relies on chloride rather than sodium and so it is not sodium 10:57 dependent 10:58 like the proximal convoluted tubule. Finally within the distal convoluted tub 11:03 ule and the 11:04 collecting duct there are many channels which basically exchange sodium and 11:09 potassium and 11:09 not necessarily ATP dependent. Rather it is controlled by an important hormone 11:16 called 11:16 aldosterone. Aldosterone is a hormone produced and secreted by the adrenal 11:22 glands, specifically 11:24 the adrenal cortex in response to low blood pressure. An increase in 11:30 circulating aldosterone 11:31 means more sodium will be reabsorbed which means more water will be reabsorbed 11:37 to increase 11:38 blood pressure. However this means more potassium will also be secreted. There 11:45 is a decrease 11:46 in potassium reabsorption which will cause hypokalemia, low potassium into 11:53 blood. Finally 11:54 let us focus on what happens only in the collecting ducts. The apical surface 12:01 of the 12:01 cells here lining the collecting ducts have these special channels called aqu 12:06 aporins which 12:07 allow for reabsorption of water. This is the final concentrating area for urine 12:13 which 12:13 occurs in the collecting duct. When the body reabsorbs water it will increase 12:19 the osmolality 12:21 of urine so it will increase the solute concentration in urine. The number of 12:27 aquaporins in the 12:28 collecting duct is controlled also by a hormone and this hormone is called ant 12:33 idiuretic hormone 12:34 also known as vasopressin. This hormone targets the collecting ducts and 12:39 essentially tells 12:40 the cells here to make more aquaporins which means with more aquaporins it 12:44 means more 12:45 water will be retained in circulation. After all the reabsorption and secretion 12:52 that takes 12:52 place along the tubule of the nephron urine is produced. So what is in urine 12:59 then? Well 13:00 it is mainly water but it also contains nitrogenous waste which is toxic if it 13:05 stays in the body. 13:06 It also contains lots of metabolites and also can contain red blood cells and 13:10 white blood 13:11 cells usually in extremely low numbers. However red blood cells and white blood 13:16 cell numbers 13:16 in urine can obviously be high but this is of course when there is an infection 13:21 or some 13:21 form of pathology that is occurring along the urinary tract.