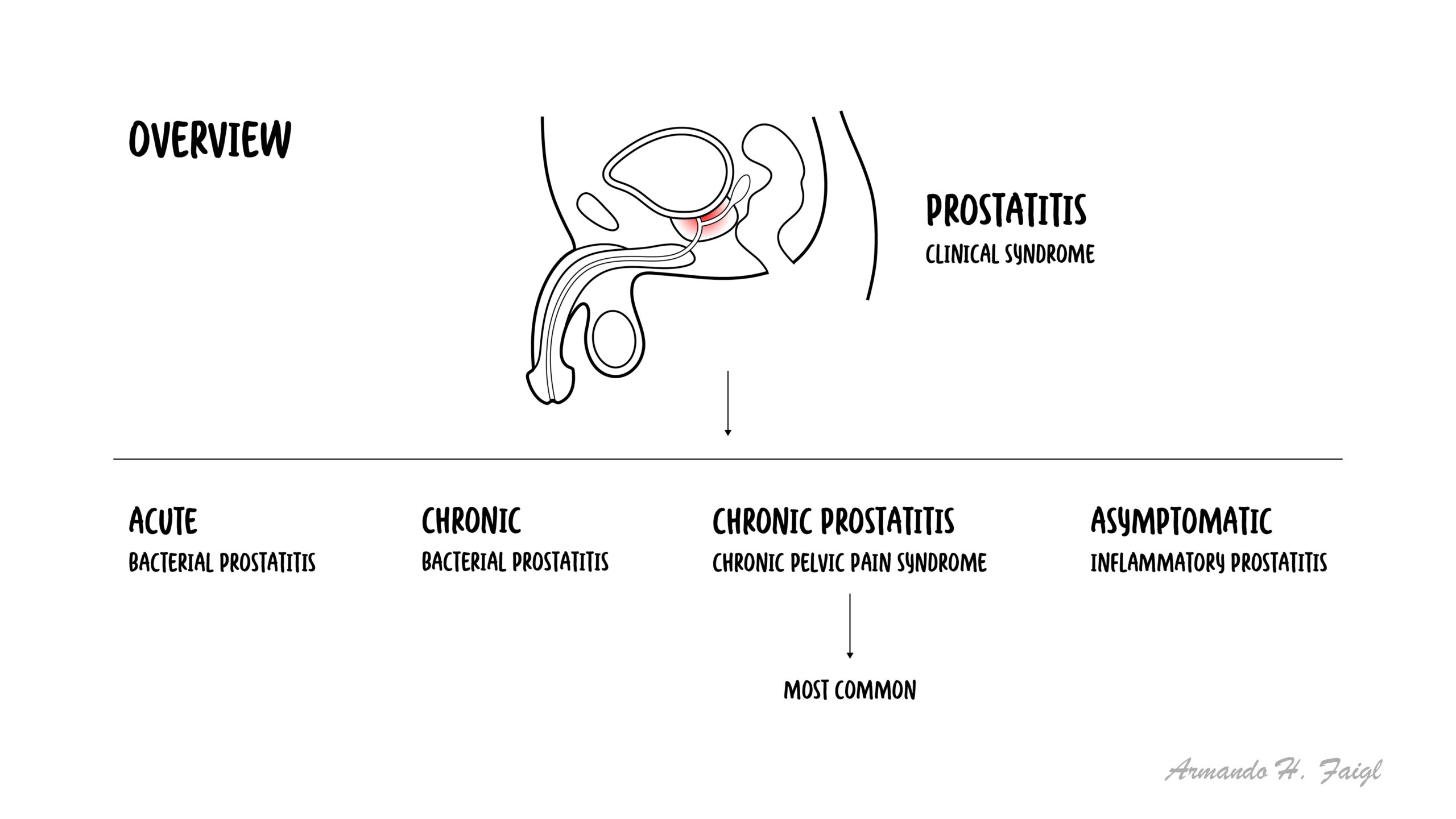
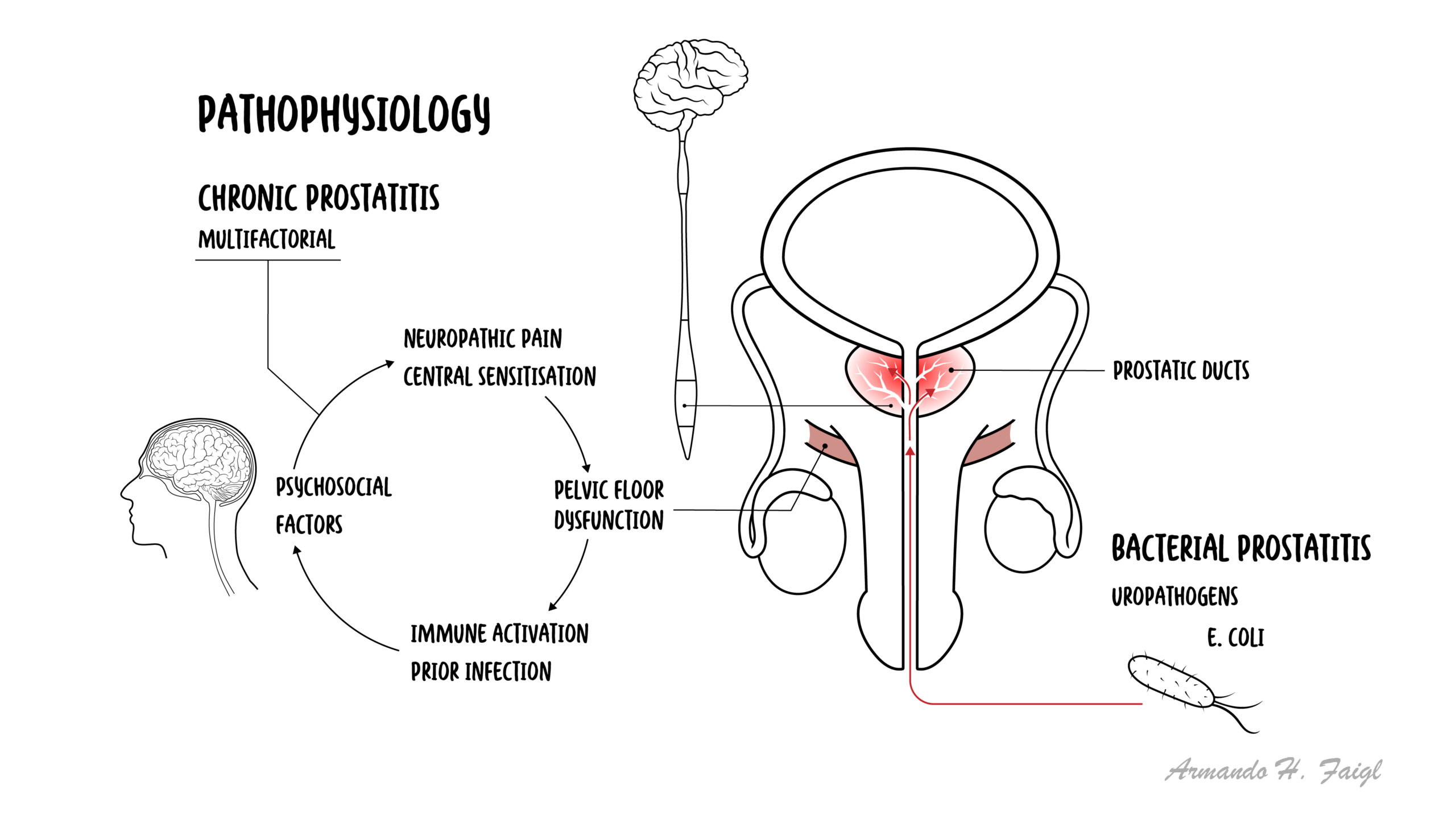
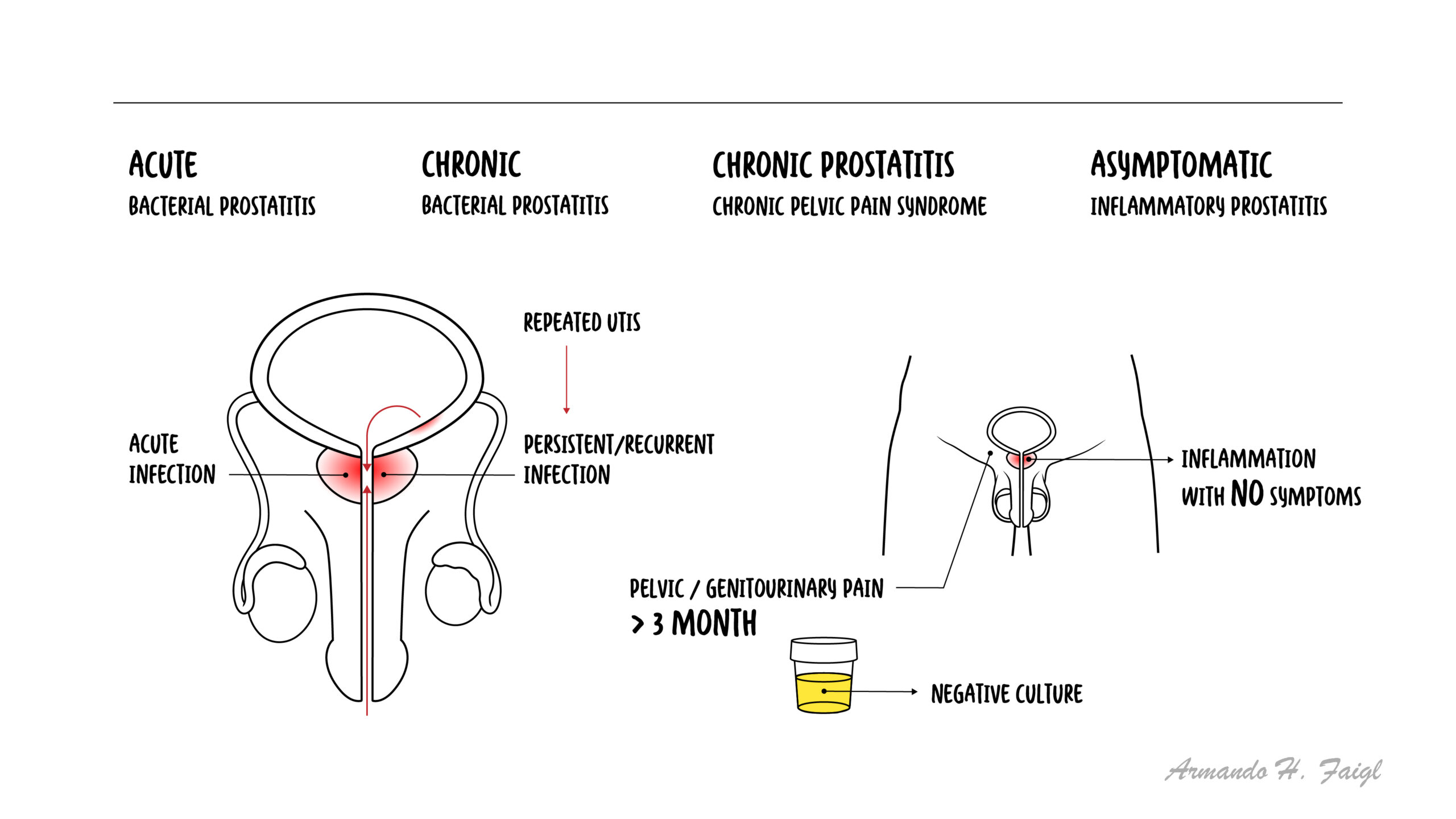
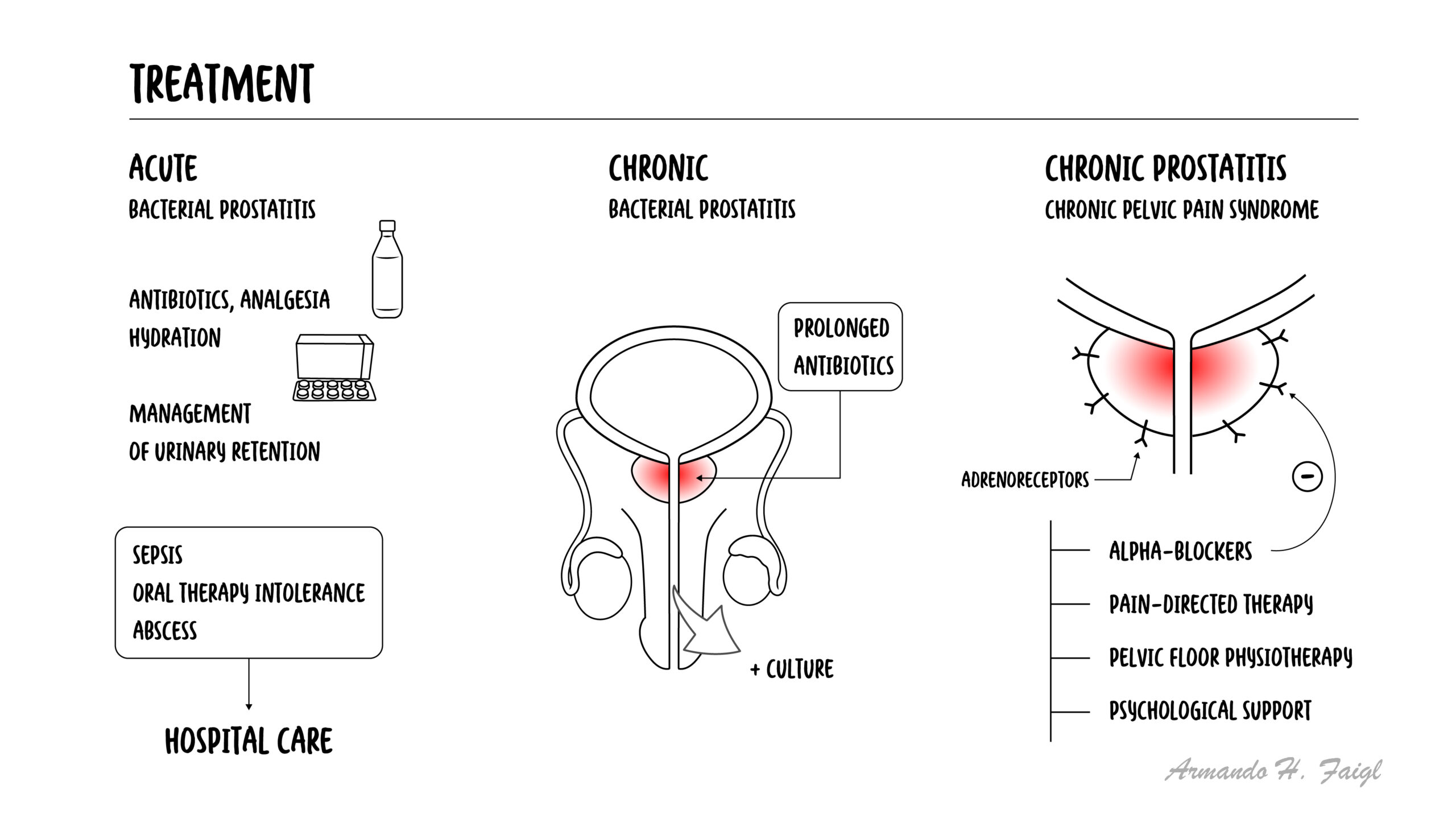
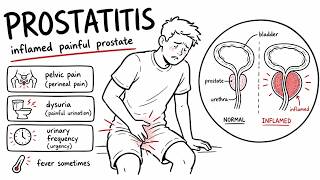
Prostatitis refers to a spectrum of conditions involving inflammation of the prostate gland, ranging from acute bacterial infection to chronic pelvic pain syndromes. It is a common urological condition affecting men of all ages, particularly those aged 30–50 years. The National Institutes of Health (NIH) classifies prostatitis into four categories: acute bacterial, chronic bacterial, chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), and asymptomatic inflammatory prostatitis. Acute bacterial prostatitis is usually caused by gram-negative organisms such as E. coli, while CP/CPPS is the most common subtype and is often non-infectious.
Definition
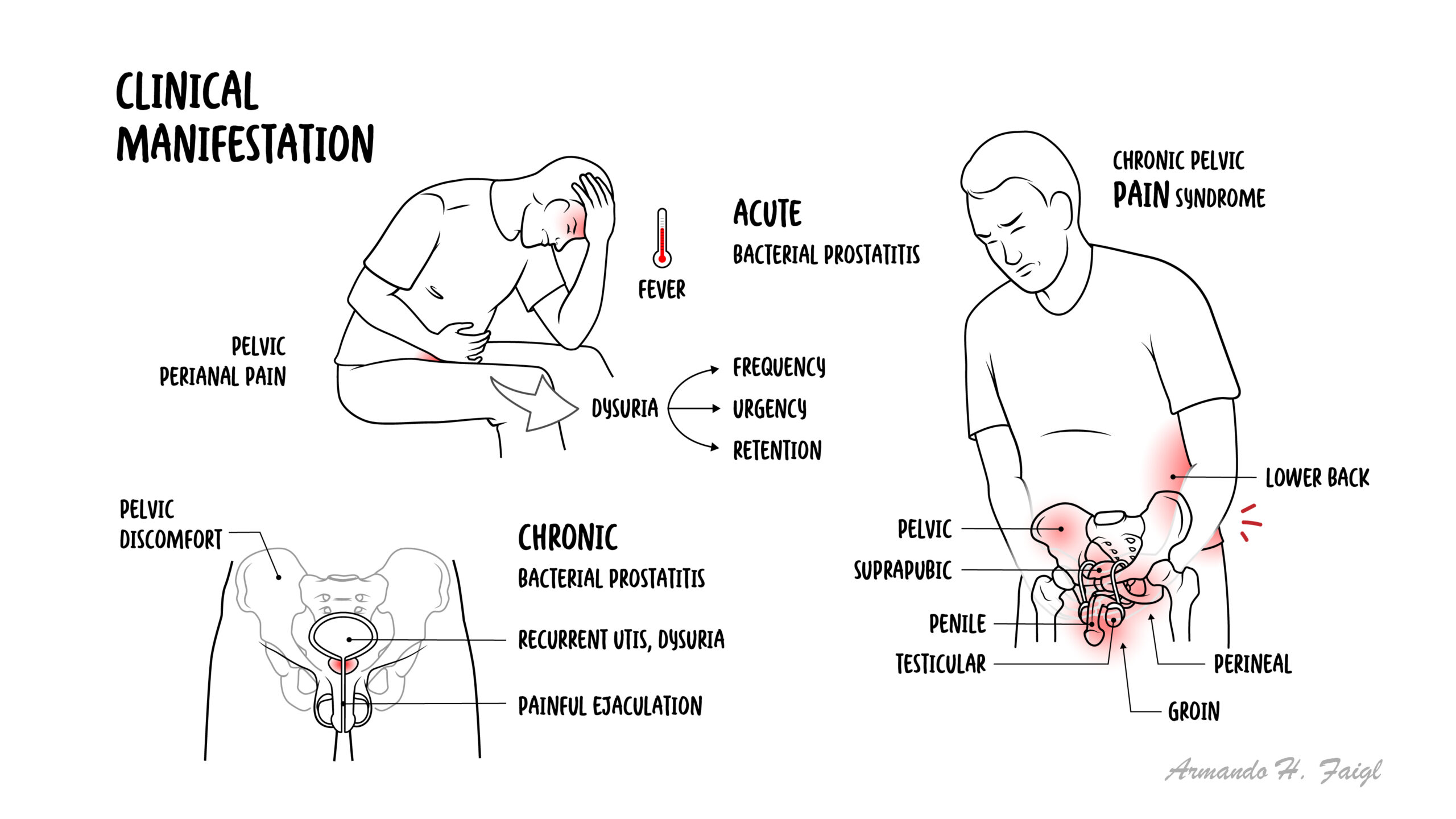
Prostatitis: Inflammation of the prostate gland. Acute bacterial prostatitis: Sudden infection of the prostate with systemic symptoms. Chronic bacterial prostatitis: Recurrent bacterial infection of the prostate. Chronic pelvic pain syndrome (CP/CPPS): Chronic pelvic pain without clear infection. Asymptomatic inflammatory prostatitis: Inflammation without symptoms.
Most prostatitis cases = non-bacterial (CP/CPPS).
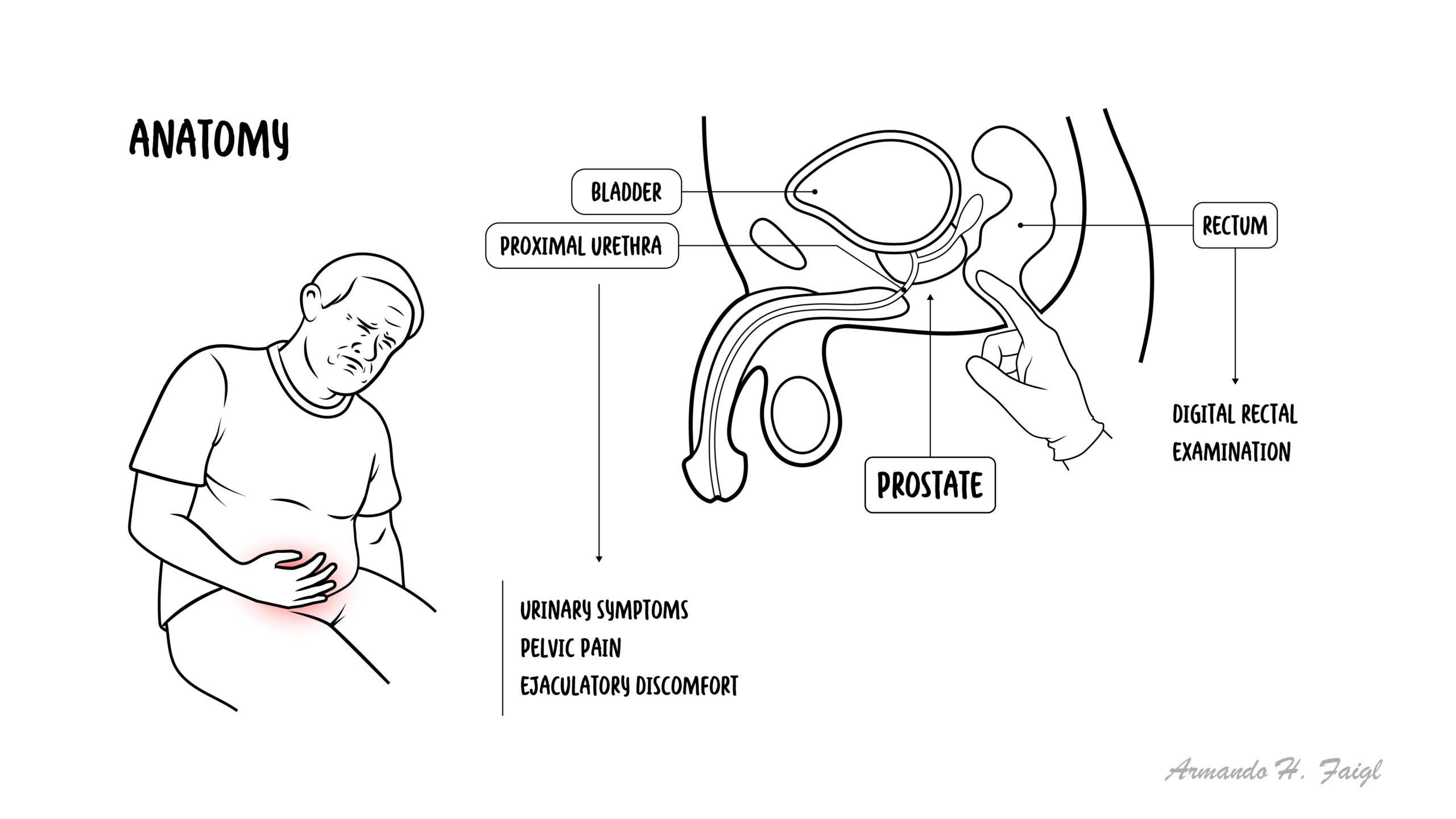
Anatomy & Physiology
Prostate gland: Located below bladder, surrounds urethra
Function: Produces prostatic fluid contributing to semen















Discussion