Non-Hodgkins Lymphoma

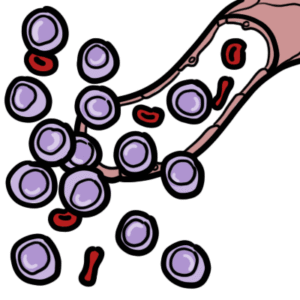
Non-Hodgkin lymphoma (NHL) is a heterogeneous group of lymphoid malignancies arising from B cells, T cells, or natural killer (NK) cells, characterised by clonal proliferation of lymphocytes at different stages of differentiation. It accounts for approximately 4–5% of all cancers worldwide, with incidence increasing with age and a median diagnosis in the sixth to seventh decade. B-cell lymphomas represent ~85–90% of cases. NHL encompasses a wide clinical spectrum from indolent (e.g., follicular lymphoma) to aggressive (e.g., diffuse large B-cell lymphoma) and highly aggressive subtypes (e.g., Burkitt lymphoma). Risk factors include immunosuppression, infections (EBV, H. pylori, HIV), autoimmune disease, and environmental exposures.
Lymphoma: Malignancy of lymphocytes arising from lymphoid tissues.
Non-Hodgkin lymphoma: Group of lymphoid malignancies excluding Hodgkin lymphoma, lacking Reed-Sternberg cells.
B-cell lymphoma: Malignancy derived from B lymphocytes (~85–90% of NHL).
Indolent vs aggressive lymphoma: Classification based on growth rate and clinical behaviour.
NHL is a spectrum of diseases, not a single entity.
Risk Factors
Chronic immune stimulation → increased risk of malignant transformation.
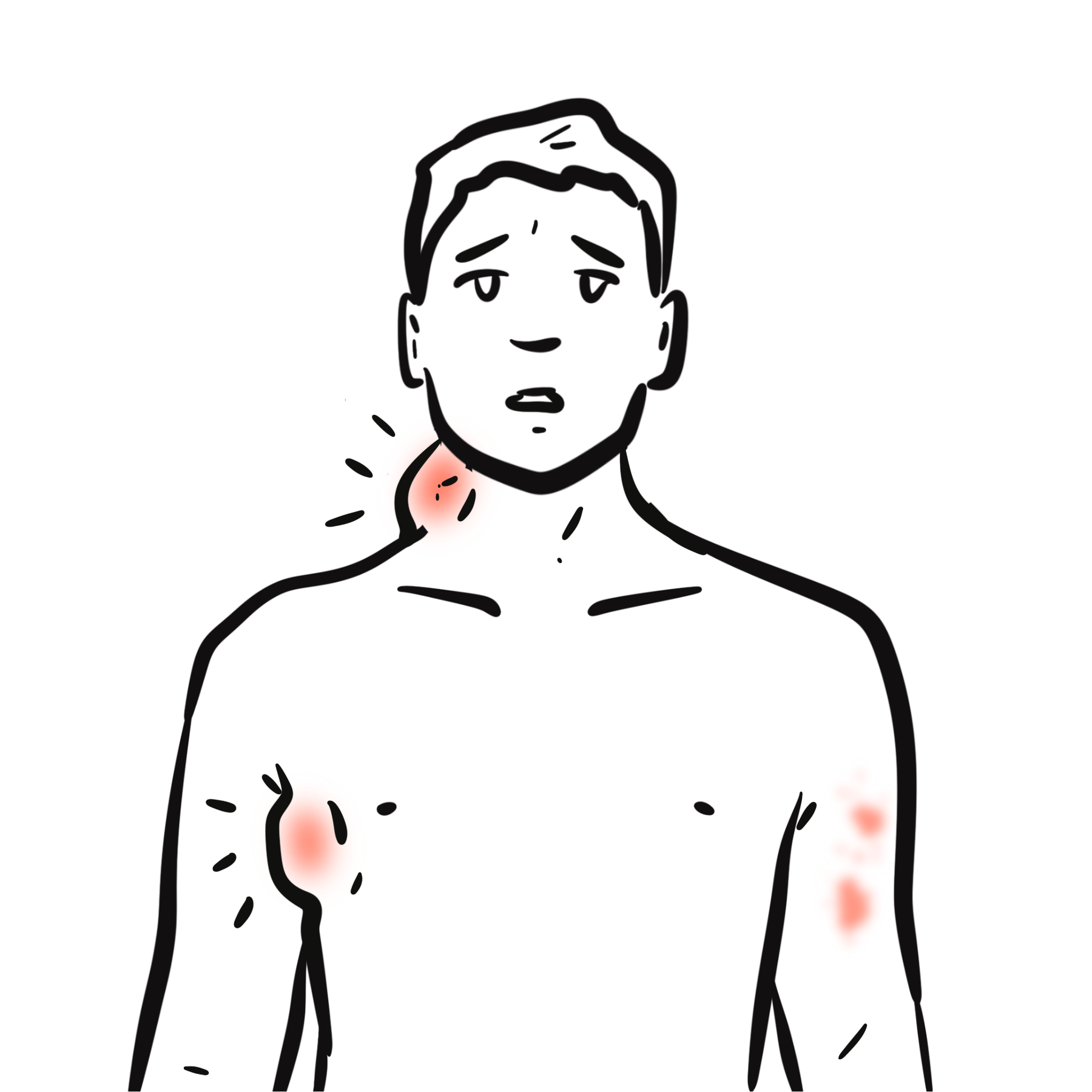
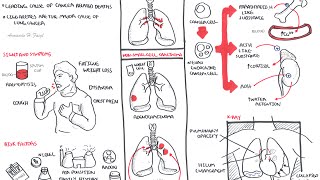
Non-Hodgkin lymphoma is more likely than Hodgkin lymphoma to present with extranodal involvement and can have a very variable clinical presentation.
Diagnostic Criteria (WHO classification 2016+ / ICC 2022):
Excisional biopsy > FNA. Excisional biopsy is preferred over FNA in suspected lymphoma because it preserves lymph node architecture, enabling accurate classification and definitive diagnosis.
By Cell Type:
By Behaviour:
Table – Common Subtypes
| Subtype | Behaviour | Key Feature |
| DLBCL | Aggressive | Most common NHL |
| Follicular lymphoma | Indolent | t(14;18), BCL2 |
| Burkitt lymphoma | Highly aggressive | MYC translocation |
| Mantle cell lymphoma | Aggressive | Cyclin D1 overexpression |
Treatment depends on type of NHL and disease burden
Always assess risk of tumour lysis syndrome, infection, hepatitis B reactivation, fertility issues, and cardiac function before treatment.
Rituximab is used for CD20-positive B-cell lymphomas.
R-CHOP = rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone.
| Treatment Overview | |
| NHL type | Usual first-line approach |
| Diffuse large B-cell lymphoma (DLBCL) | R-CHOP or similar chemoimmunotherapy; aggressive but potentially curable |
| Follicular lymphoma, asymptomatic low burden | Watch and wait |
| Follicular lymphoma, symptomatic/high burden | Anti-CD20 therapy ± chemotherapy, e.g. rituximab-based treatment |
| Burkitt lymphoma | Urgent intensive multi-agent chemotherapy + CNS prophylaxis |
| Mantle cell lymphoma | Immunochemotherapy ± BTK inhibitor; transplant considered in fit younger patients |
| Marginal zone lymphoma | Treat cause if present, e.g. H. pylori eradication in gastric MALT; radiotherapy or rituximab-based therapy if persistent/disseminated |
| Relapsed/refractory aggressive B-cell NHL | Salvage therapy, CAR-T, bispecific antibodies, or transplant depending on fitness and prior response |













Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion