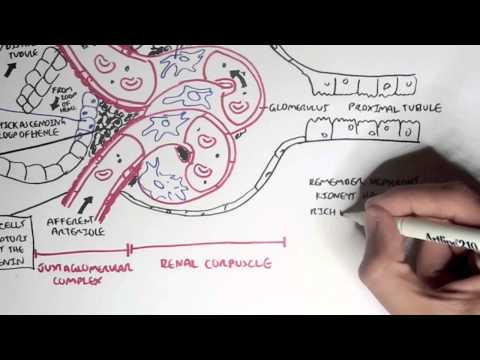
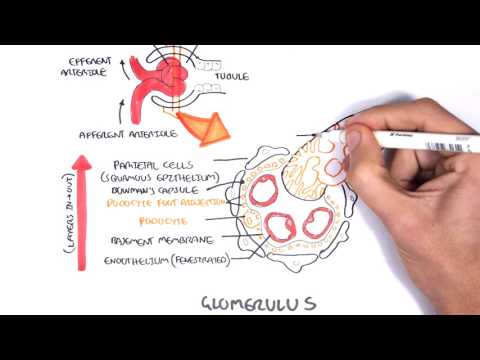
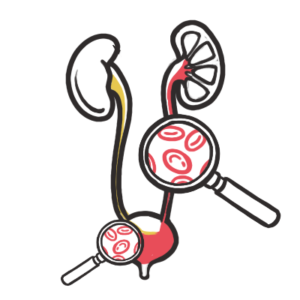
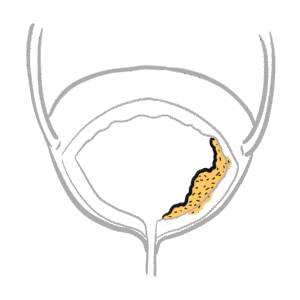
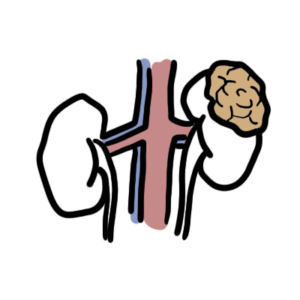
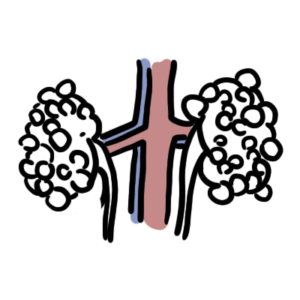
0:00 Hello. In this video, we're going to look at hematuria, which is the presence 0:08 of red 0:08 blood cells or blood in urine, hematuria. And essentially, in this video, we're 0:14 going 0:15 to look at the causes of hematuria. So, if someone presents with hematuria, 0:19 what are 0:19 the differential diagnoses? Before we talk about some of the causes of hemat 0:24 uria, let 0:24 us recap the urinary system between the male and the female and the anatomy. So 0:32 , 0:32 here is the male and here is the female. So, in the male, we have the penis, 0:37 the 0:37 prostate, the bladder, urita, the kidneys, and the adrenal glands. The urogen 0:45 ital 0:45 diaphragm here separates the prostate and the penis. So, here is the internal 0:51 urethral sphinctum at the neck of the bladder and then you have the external 0:56 urethral sphinctum along where the urogenital diaphragm is. And then, obviously 1:03 , the 1:03 end of the penis is the external urethral meatus, where urine comes from or 1:08 sperm, 1:08 depending on what you're doing. All right. So, that was the males. Let's look 1:12 at 1:12 the female now. So, here we have the urethral opening, where urine comes from, 1:19 and vaginal opening and for sexual activity. And here is the 1:28 fallopian tube for the reproductive system and the ovary, where the eggs are. 1:36 And here, I'm cutting a section because on this side, this is the uterus. And 1:42 essentially, the fallopian tube comes from the uterus. And I'm drawing the 1:46 uterus here and the reproductive system, which is the fallopian tube and ovary, 1:52 because some differential diagnosis of hematuria, you know, affect these 1:59 structures. All right. So, that was the male and female urinary system. Now, 2:06 let's 2:06 just look at the porters of hematuria now. And let's just use the male system 2:13 here, male urinary system. So, if someone presents with hematuria, it's 2:16 important 2:16 to ask them, do they notice the blood when they stop peeing or at the end of 2:21 the peeing or throughout? So, if hematuria occurs initially or on 2:27 terminal voiding, like at the end of peeing, the site of bleeding or the 2:32 cause is probably from the neck of the bladder down. Whereas, if the hematuria 2:38 happens from start to finish, so total hematuria, the bleeding may most would 2:45 most likely originate from the bladder or from the kidneys. So, I hope that 2:51 made 2:52 sense. Now, some differential causes, different differential diagnosis for 2:56 hematuria include recent urological intervention, such as bladder catheter 3:01 ization, 3:02 indwelling urethral stent or a prostate biopsy, a recent prostate biopsy, and 3:10 prostate biopsy. Obviously, another differential for hematuria would be 3:14 non-prosthetic hyperplasia. And of course, infection of the bladder could cause 3:21 hematuria. So, this is known as uteritis. Uteritis can lead to infection of the 3:27 kidneys itself. And this is referred to as pylonephritis. Trauma to the kidneys 3:32 or 3:33 the ureter or the bladder or the penis itself can lead to hematuria. 3:38 Obviously, cancer or growth's tumours in the kidneys or anywhere along the 3:46 urological system can lead to hematuria. Of course, the functional units of the 3:52 kidneys itself, which are the nephrons, things can cause problems in the neph 3:59 ron, 4:00 specifically can lead to hematuria. So, a very common condition is known as 4:04 glomerular nephritis or any nephropathy for that sake. And causes of 4:10 glomerular nephritis include infections, toxins, such as drugs. Oter antibodies 4:17 , 4:17 so autoimmune disease, diabetes and hypertension could also lead to glomerular 4:22 nephritis, which is a differential diagnosis for hematuria. 4:28 Nefrolithiasis is kidney stones. So, kidney stones could lead to hematuria. And 4:36 then 4:36 you have obviously kidney stones that actually lodge in the ureter itself. And 4:42 this is known as urolithiasis. Urolithiasis, which are kidney stones in the ure 4:49 ter, 4:49 are formed by calcium oxalate most of the time. And they lodge in specific 4:54 sites within the ureter, mainly the beginning, middle and end. So, these are 5:01 the sites of actually sites of contraction of the ureter. And that's why 5:04 the kidney stones most often lodge there. So, the beginning part is known as a 5:11 pelvic ureteric junction. Then the middle part is a pelvic brim. The third part 5:16 , 5:16 which where the ureter enters the urinary bladder, is a vesico ureteric 5:20 junction. 5:21 Another differential diagnosis for hematuria is a genetic disorder known as 5:30 polycystic kidney disease. And this disease forms cysts around the kidneys, 5:36 which could result in blood upon your nation. Now, specifically for the female 5:41 patient, there are some diseases or some common problems that occur for 5:48 differential of hematuria. And this includes endometriosis, which is the 5:52 growth of eutrine cells elsewhere in the body. And also, there's a pseudo 5:59 hematuria where it's actually just with a female experience, where a female 6:04 person experiences their normal menstrual cycle, so mensus, or a recent 6:09 intercourse causing bleeding in the re-reproductive system can lead to 6:14 bleeding, possible bleeding on your nation, because of trauma to the area. 6:20 Recent vigorous activity can induce hematuria. And lastly, coagulopathies can 6:26 also cause hematuria because the person is unable to clot properly. That's the 6:31 presence of blood in the urine. So, that was some of the causes and 6:36 differential diagnoses of hematuria. Now, what are some investigations that can 6:41 be performed? If someone presents with hematuria, what investigations would you 6:45 order? So, some investigations include a full blood count. Full blood count is 6:50 to 6:50 see if the person is anemic and to check for the presence of white blood cells, 6:53 the numbers, and high numbers would obviously indicate infection. Then you 6:58 also have urine dipstick. Urine dipstick, you can then use it to have a 7:04 microscopic examination of the urine and also culture the urine to see if any 7:10 signs of infection, bacterial growth. Then you can also perform coagulation 7:16 studies, so to check if the patient has any coagulopathies. You can also 7:22 perform a 7:23 urinary bladder cancer marker. And usually people the age of 40 who 7:27 presents with hematuria, you should always rule out cancer of the bladder 7:34 because this is often how cancer of the bladder presents and it's often most 7:39 often in people over the age of 40. And then you can also do a PSA and this is 7:45 to this is prostate-specific antigen, so this is a check for any APH or any 7:50 possible prostate cancer. And then finally you can also perform a CT or 7:57 ultrasound and these are imaging studies to see how the kidney looks like. With 8:02 these techniques you can see the presence of cysts, yes, such as in 8:07 polycystic kidney disease. And these investigations are essentially there to 8:13 help you rule in diseases and rule out some differential diagnoses. So I hope 8:18 this video made sense and I hope you enjoyed it. Thank you for watching.