Hyperlipidaemia

Hyperlipidaemia is an umbrella term which encompasses genetic and acquired disorders that raise lipid levels within the blood. Hyperlipidaemia does not independently cause clinical symptoms, rather can lead to other disorders that can manifest in possible life-threatening presentations. Most notably, hyperlipidaemia causes atherosclerosis which may lead to cardiovascular, cerebrovascular, and peripheral vascular disease.1
Objectively, hyperlipidaemia can be defined as the following levels being in the 90th percentile or greater in comparison to the general population:
Or if the high-density lipoproteins (HDL) levels are less than the 10th percentile in comparison to the general population.
Hyperlipidaemia: elevated levels of lipids in the blood, including cholesterol and/or triglycerides. Increases cardiovascular risk. (In Australia total cholesterol > 5.5 mmol/L or triglycerides > 2.0 mmol/L.)
Hypertriglyceridaemia: Triglyceride levels in the blood are raised, due to genetic, metabolic, or lifestyle factors. It increases the risk of pancreatitis and may contribute to cardiovascular disease. (In Australia fasting triglycerides > 2.0mmol/L.)
Hypercholesterolaemia: elevated level of cholesterol in the blood, typically referring to high low-density lipoprotein (LDL) cholesterol, which is a major risk factor for atherosclerotic cardiovascular disease. (In Australia, total cholesterol > 5.5 mmol/L or LDL-C > 3.5 mmol/L.)
Lipoproteins: spherical particle made up of lipids (fats) and proteins (apolipoproteins) that transports cholesterol, triglycerides, and other fats through the bloodstream.
Triglycerides
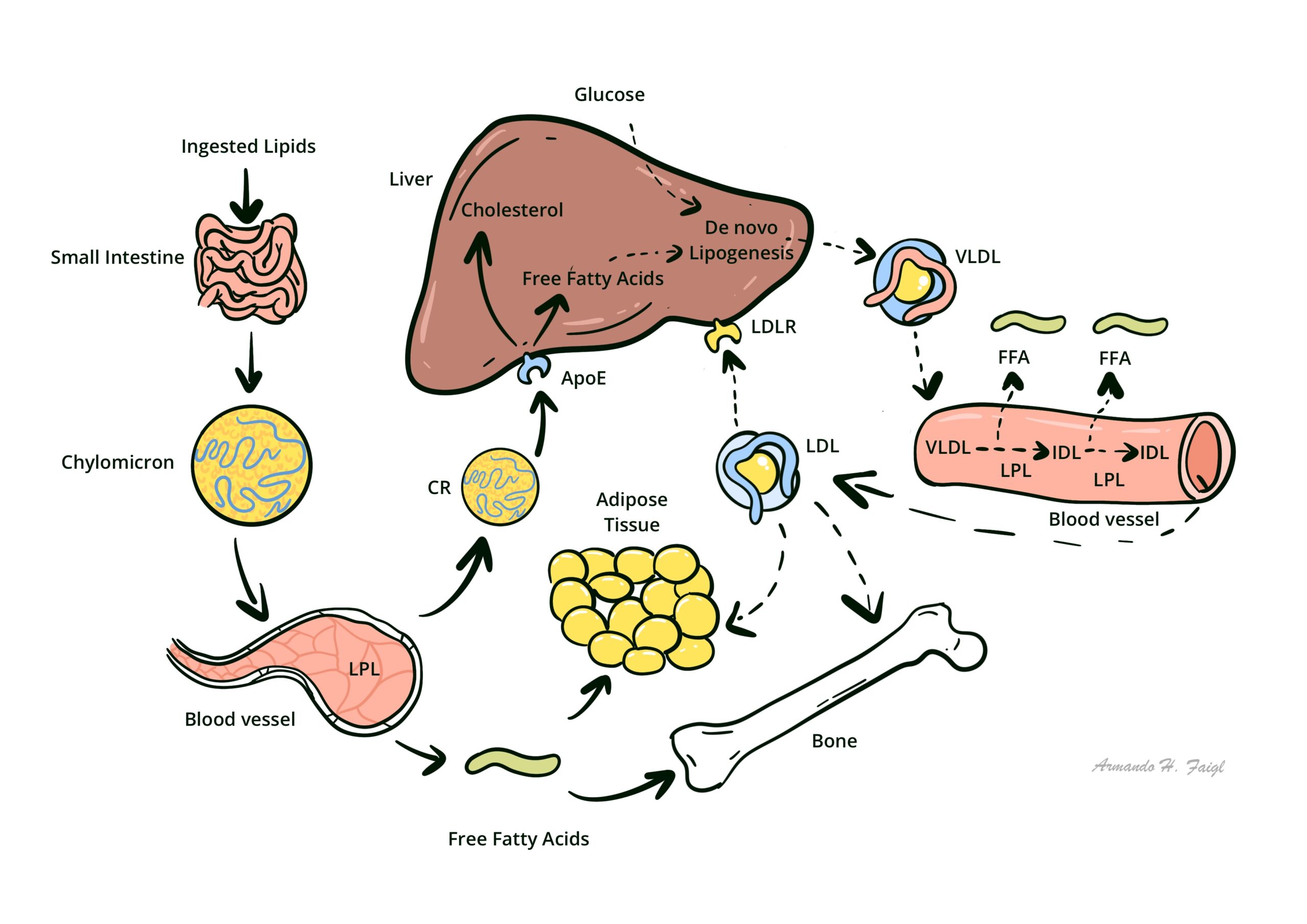
Triglycerides are the main form of stored energy in the body. They consist of three fatty acids attached to a glycerol backbone. Triglycerides are packaged into chylomicrons (from the intestine) and VLDL (from the liver) for transport through the blood. They are broken down by lipoprotein lipase at tissues to release fatty acids for energy use or storage.
Cholesterol
Cholesterol is a key structural component of cell membranes, providing fluidity and stability. It is also the precursor for steroid hormones, vitamin D, and bile acids. Cholesterol in the blood comes from dietary intake and hepatic synthesis. It is transported mainly in LDL (delivers cholesterol to tissues) and HDL (returns excess cholesterol to the liver for excretion).
After a meal, chylomicrons carry dietary triglycerides and cholesterol through the lymphatics into the bloodstream. The liver produces VLDL to export triglycerides. LDL arises from VLDL remnants and delivers cholesterol to tissues. HDL collects excess cholesterol for return to the liver (reverse cholesterol transport).
Primary (genetic) hyperlipidaemia
Inherited disorders of lipid metabolism (e.g. familial hypercholesterolaemia, familial combined hyperlipidaemia)
Primary Hyperlipidaemia will be covered in more detail separately
Secondary hyperlipidaemia
Due to other conditions or risk factors, including:
– Diabetes mellitus
– Hypothyroidism
– Nephrotic syndrome
– Excess alcohol intake
– Obesity
– Certain medications (e.g. corticosteroids, antiretrovirals)
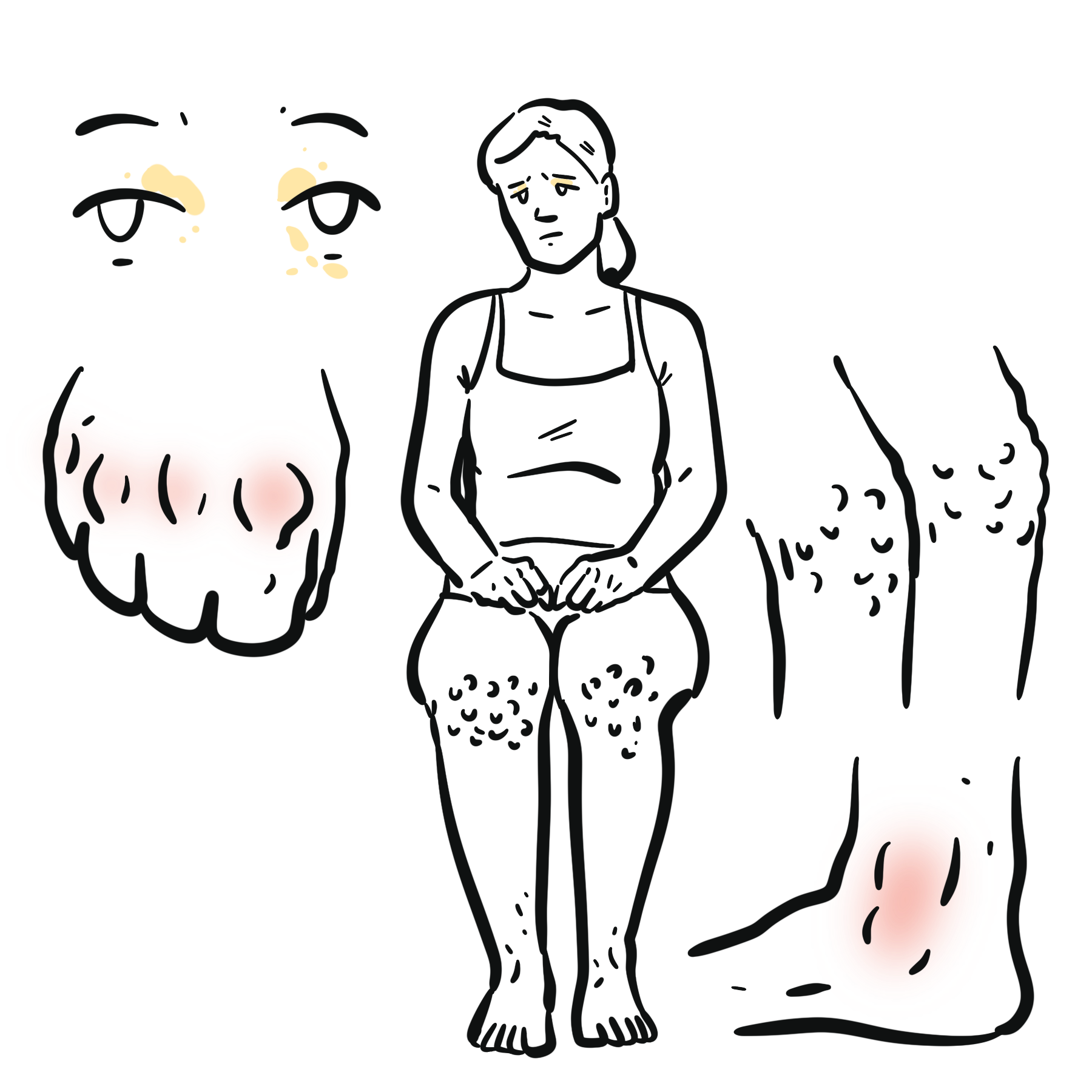
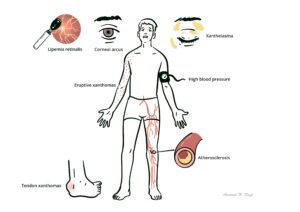
Familial hyperlipidaemia presents early with high LDL-C (>5 mmol/L), premature cardiovascular disease, tendon xanthomas, corneal arcus in young patients, or a strong family history.
Risk factors
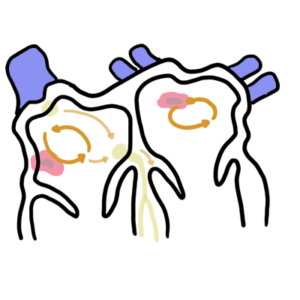
Increased levels of lipids in the blood make a person at increased risk for atherosclerosis. Atherosclerosis develops through the continuous growth of lipid lesions within the arterial wall (intimal layer) which results in chronic inflammation. The development of atherosclerosis is like so:
LDL uptake and oxidisation
Endothelial dysfunction
Numerous factors can induce endothelial dysfunction including:
Adhesion of lymphocytes and monocytes
Foam cell formation fatty streak formation
Fatty streak early fibroatheroma formation
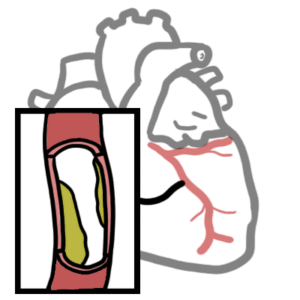
Late fibroatheroma formation
Complications of hyperlipidaemia
Hyperlipidaemia
Management of hyperlipidaemia is determined through the cardiovascular risk calculator, taking into consideration investigations as well as pertinent points of their lifestyle and demographic9.
This calculator can be found here: https://www.cvdcheck.org.au/calculator
Desirable parameters in Australia
Non-fasting samples can falsely elevate triglycerides.
Elevated triglycerides >10 mmol/L → risk of pancreatitis.
Exclude secondary causes before starting long-term lipid therapy: Check TSH, fasting glucose/HbA1c, liver function, renal function, and urine ACR (albumin:creatinine ratio).
Lifestyle improvements
Other medications that may be suggested to lower lipid levels: Fibrates, Niacin, Omega-3 fatty acid supplement.
Combination therapy (statin + ezetimibe ± PCSK9 inhibitor) may lower LDL-C by >80%.
Target














Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.

Discussion