Acute Heart Failure


Heart failure is a condition in which the heart does not pump enough blood to meet all the needs of the body. It is caused by heart muscle damage or dysfunction, valve problems, heart rhythm disturbances and other rarer causes. Acute heart failure can present as new-onset heart failure in people without known cardiac dysfunction, or as acute decompensation of chronic heart failure. Acute heart failure is a common cause of admission to hospital.
Heart failure: Reduced CO and/or elevated intracardiac pressures at rest or during stress. Caused by a structural and/or functional cardiac abnormality
Acute heart failure: Describes a patient with acute-onset dyspnoea and pulmonary oedema, but can also apply to cardiogenic shock where the patient is hypotensive and oliguric.
Acute decompensated heart failure: Defined as the sudden or gradual onset of the signs or symptoms of heart failure (usually person with chronic heart failure) requiring unplanned office visits, emergency room visits, or hospitalization.
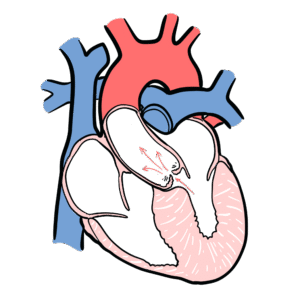
Factors influencing Cardiac Output
The four determinants of Cardiac Output are preload, afterload, heart rate and contractility.
Most commone cause of acute heart failure (Severe pulmonary oedema is usually left ventricular failure (post MI), valvular heart disease, arrhythmia and ARDS.
| Causes | Examples |
| Coronary artery disease (Most common cause) | Post MI |
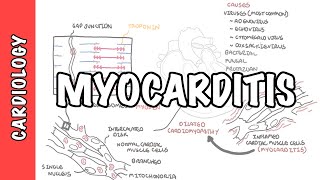
| Infection | Systemic sepsisMyocarditis |
| Mechanical | EndocarditisPulmonary emboliValve problemsSeptal defectsTamponade |
| Drugs | B-BlockersCalcium antagonistsCytotoxic therapy |
| Hypoxaemia | |
| Metabolic | AcidaemiaThiamine deficiencyHypocalcaemiaHypophosphataemia |
| Myocardial contusion | Blunt thoracic trauma |
| Myocardial infiltration | TumourSarcoidosisAmyloidosis |
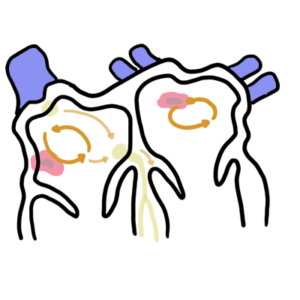
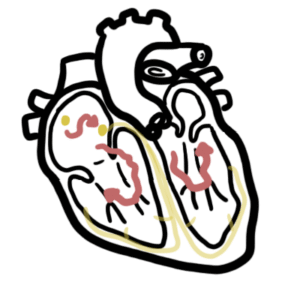
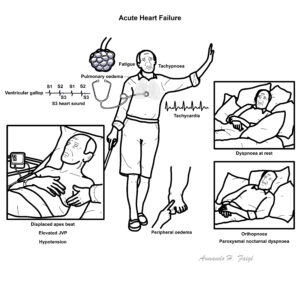
Acute heart failure is most often caused by a cardiac problem such as following a MI. The diagram below illustrates what happens following an MI and the bodies response to these changes.
Cardiogenic shock
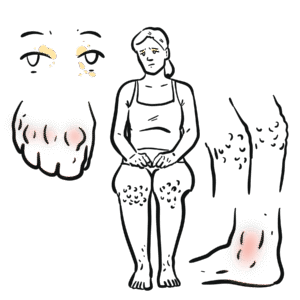
Symptoms
Has there been any drugs recently given of other illnesses that could cause these symptoms.
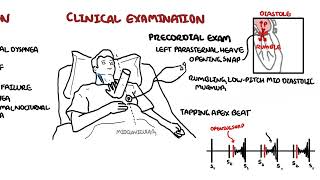
Signs
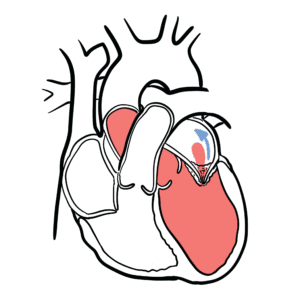
The third heart sound (S3), also known as the “ventricular gallop”, occurs just after S2 when the mitral valve opens allowing passive filling of the left ventricle. The S3 sound is actually produced by the large amount of blood striking a very compliant left ventricle (systolic heart failure meaning dilated ventricles). Remember S3 can be a normal finding in children, pregnant females, and well trained athletes, however a S4 heart sound is almost always abnormal.
Acute heart failure has an underlying cause. Other then finding what the cause is, it is important to keep differentials below in mind.
Serology
Imaging
Resuscitation – Begin treatment before investigations
Once stable and improving
| ANTIHYPERTENSIVE DRUGS | ||
| Drug Class | MOA | Adverse effects (Contraindications) |
| ACE Inhibitors | Angiotensin converting enzyme inhibitor inhibits Angiotensin II a potent vasoconstrictor. Also prevents aldosterone release (Na+ and fluid lost and K+ retained) | Hypotension, Rash, Cough, taste disturbance, angioedema (Pregnancy, renal stenosis) |
| Beta Blockers | Worsening of the failure, severe hypotension, bradyarrhythmias (Chronic obstructive lung disease, Peripheral vascular disease) | |
| Diuretics | Inhibit the reabsorption of sodium from the nephron and so inhibits water reabsorption | |
| Nitrates | Dilates venous vessels, decreasing preload. | |
| Watch Pharmacology – Antihypertensives |
| IONOTROPIC DRUGS | ||
| Drug Class | MOA | Adverse effects (Contraindications) |
| Catecholamines (Adrenaline) | Predominately acts on alpha and beta receptors in the heartperipheral vasoconstriction (alpha adrenergic action)Positive inotropic effect on the heart and dilation of coronary arteries (beta adrenergic action) | |
| Phosphodiesterase inhibitors (Milrinone) | Competitively inhibit the phosphodiesterase III isoenzyme responsible to the breakdown of cAMP, increasing inracellular cAMP levels and improving myocardial contractility independent of beta-receptor stimulation | |
| Cardiac glycosides (Digoxin) | Slows HR and reduces AV nodal conduction by an increase in vagal tone and a reduction in sympathetic activity. Increases the force of myocardial contraction by increasing the release and availability of stored intracellular calcium | |
| Calcium and calcium sensitisers (Levosimendan) | Binds to and sensitises cTnC to calcium without raising intracellular calcium – Improves cardiac performance and contractility during systole without impairing ventricular relaxation during diastole | |
Pulmonary Oedema
| Indication for Intubation |
| Patient exhaustion |
| Declining level of consciousness |
| Increasing confusion and agitation |
| Rising partial pressure of carbon dioxide (PaCO2) |
| Failure to maintain an adequate partial pressure of oxygen (PaO2). |
| Respiratory arrest/coma |










Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.


Discussion