

Hypertension
Overview
Hypertension is defined as BP ≥140/90 mmHg. Hypertension can be divided into Primary or Secondary. The main goal of treatment is to decrease the risk of mortality and of cardiovascular and renal morbidity.
| Classification | Systole |
| Normal | 120-129 |
| High-normal | 130-139 |
| Hypertension Grade I | 140-159 |
| Hypertension Grade II | 160-179 |
| Hypertension Grade III | >180 |
The mean arterial pressure (MAP) is a term used in medicine to describe an average blood pressure in an individual. MAP is a product of cardiac output and the total peripheral resistance.
Epidemiology
- Worldwide, raised blood pressure is estimated to cause 7.5 million deaths, about 12.8% of the total of all deaths.
- Raised blood pressure is a major risk factor for coronary heart disease and ischemic as well as hemorrhagic stroke. Blood pressure levels have been shown to be positively and continuously related to the risk for stroke and coronary heart disease.
- Globally, the overall prevalence of raised blood pressure in adults aged 25 and over was around 40% in 2008.
- The proportion of the world’s population with high blood pressure, or uncontrolled hypertension, fell modestly between 1980 and 2008. However, because of population growth and ageing, the number of people with uncontrolled hypertension rose from 600 million in 1980 to nearly 1 billion in 2008.
Aetiology & Risk Factors
Risk Factors for hypertension are essentially the same for other cardiovascular diseases.
Pathophysiology
- Thickened internal elastic lamina
- Smooth muscle hypertrophy and fibrosis -> decreased wall compliance
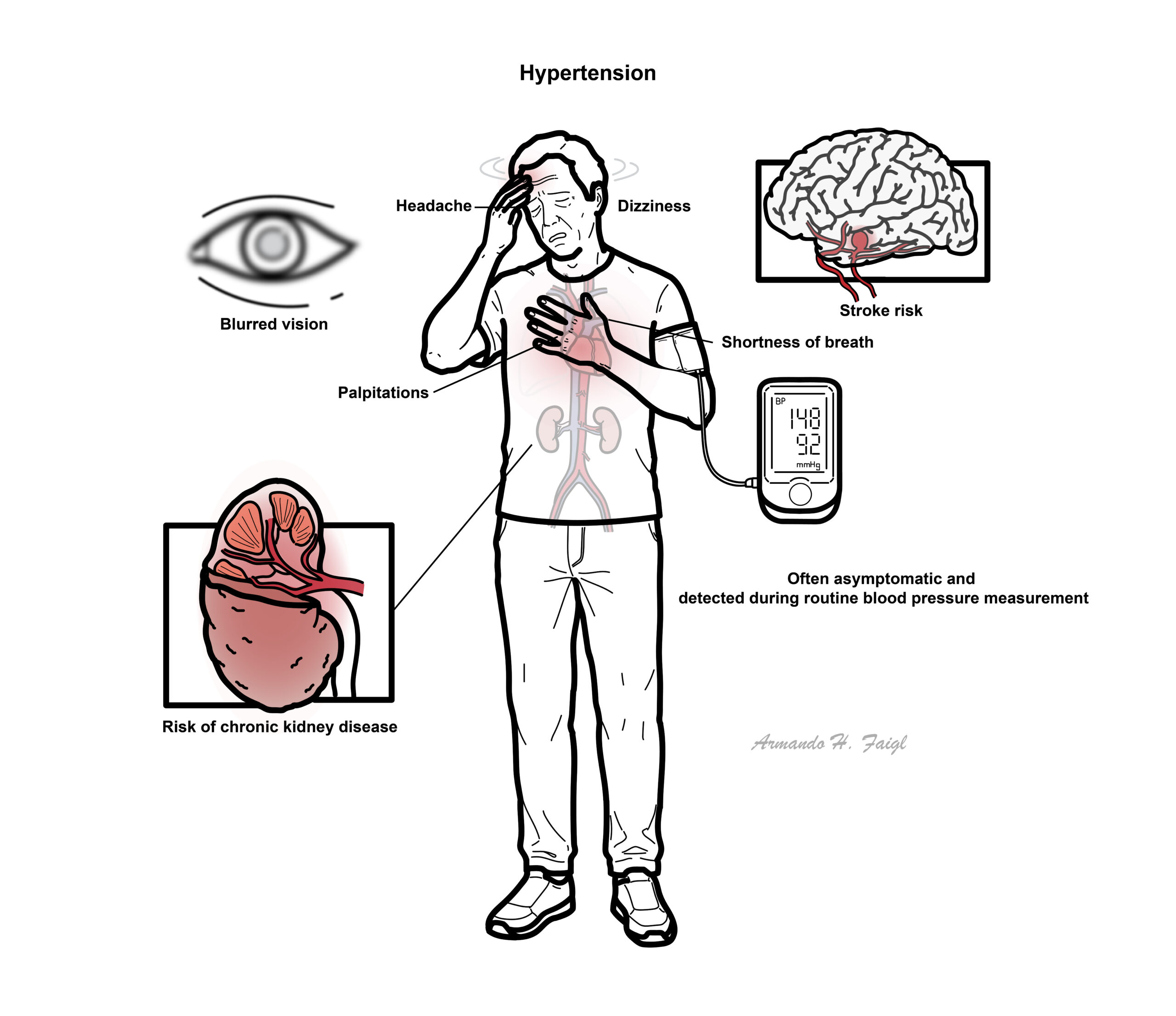
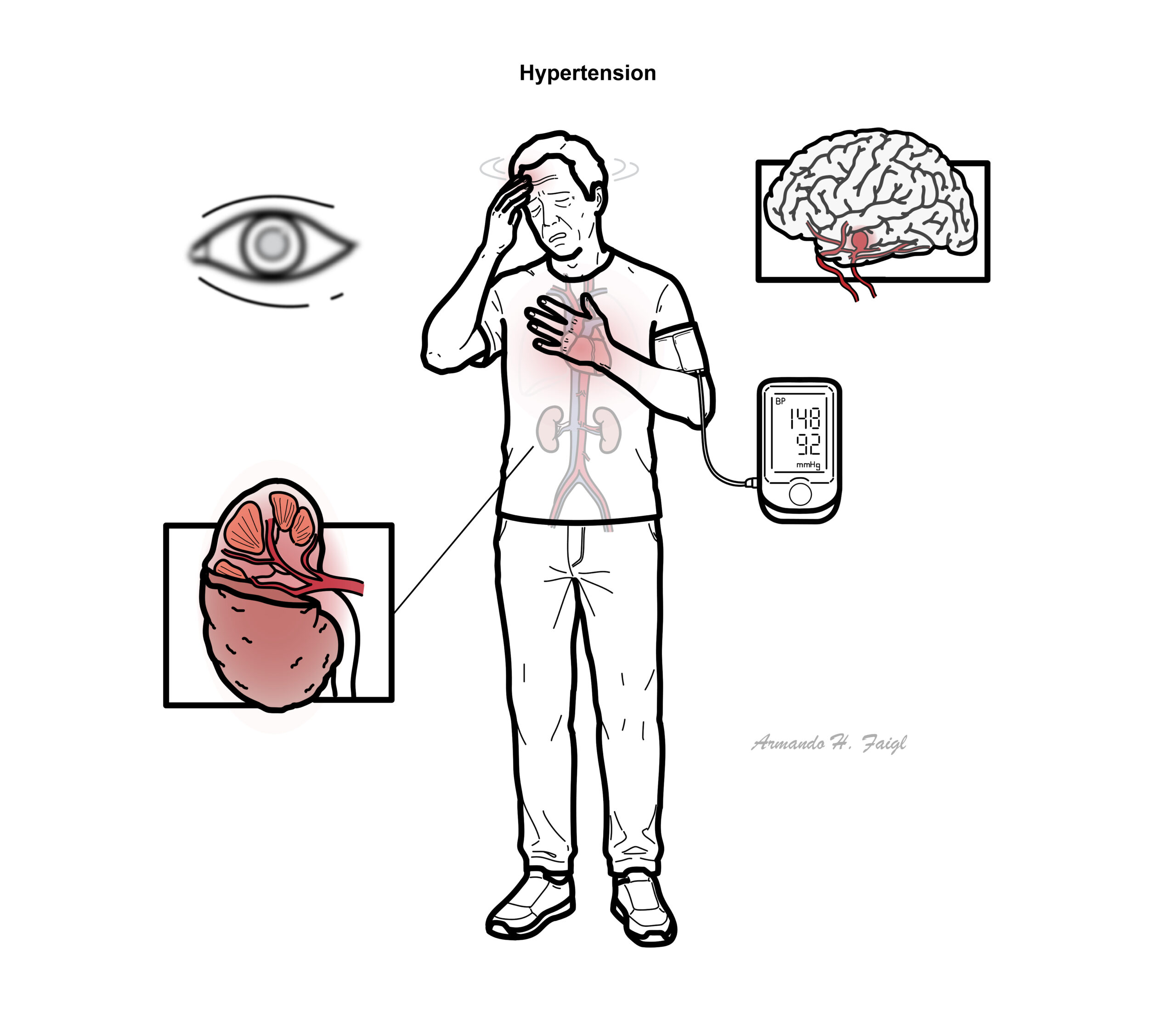
Clinical Manifestations
Hypertension is a common disorder that affects a large proportion of the community. It is usually asymptomatic and is detected on routine examination or after the occurrence of a complication such as a heart attack or stroke. It is often referred to as the silent killer.
Several things can cause bias to the hypertension readings (White coat hypertension). In the clinic, usually the 1st measurement is disregarded and the average of the second and third readings are taken.
Diagnosis
This is the most common situation, when no underlying cause can be found to account for raised blood pressure.
In a minority of cases, an underlying, often reversible cause can be found.
Vascular
- Renal Artery Stenosis
- Coarctation of the aorta
- Pre-eclampsia
Renal artery stenosis should be suspected if BP is unexpectedly low or kidney function deteriorates in patients taking an ACEI or ARB.
Kidneys
- Chronic Kidney Disease
- Nephrotic Syndrome
- Nephritic Syndrome
- Obstructive Uropathy
- Polycystic Kidney Disease
Endocrine
- Phaeochromocytoma
- Hyperaldosteronism
- Cushing’s Disease
- Hyperthyroidism
Toxic causes
- Chronic alcohol use
- Long term NSAIDs
- Oral contraceptive pill
- Illicit medication such as cocaine or Amphetamines
Pseudo-hypertension
There are many causes of hypertension. Primary hypertension is mainly a result of lifestyle and genetics. Secondary hypertension is cause by an underlying, often reversible condition (ie. renal artery stenosis, medication)
Although in the majority of patients hypertension is primary/essential, there are certain features that may lead to a suspicion of an underlying cause (secondary hypertension):Young patient (<40 years)Rapid onset of hypertensionSudden change in blood pressure readings when previously well controlled on a particular therapyResistant hypertension that is unresponsive to pharmacological therapies.
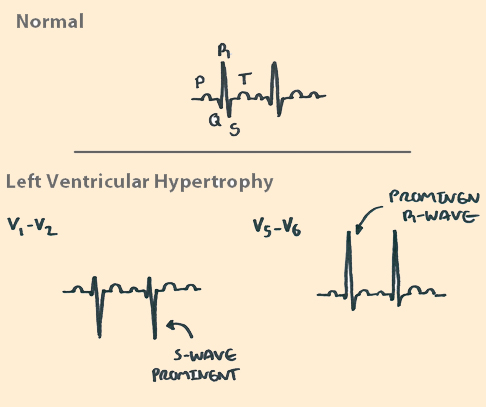
- ECG – may show evidence of LVH or old infarction
- GFR – monitor kidney function
- Fasting lipid – High fat is associated with hypertension
- Urinalysis – proteinuria many indicate end organ damage
- Hb – Anaemia may indicate CKD, polycythemia may indicate Phaechromocytoma
- Plasma renin – low renin suggests hyperaldoesteronism
- Plasma aldosterone (with hypokalaemia and high sodium) – suggests hyperaldosteronism
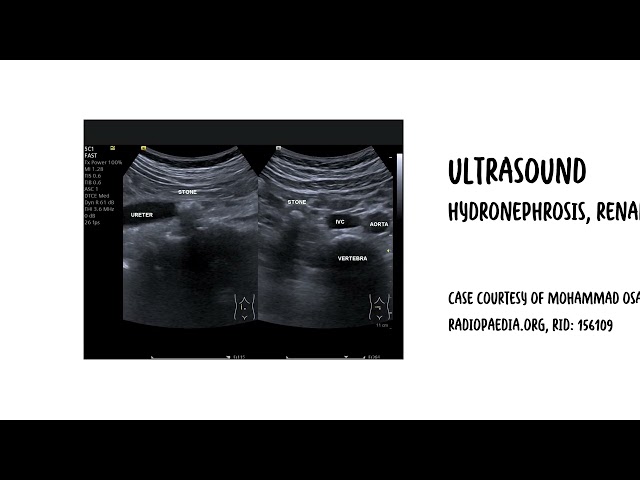
- Renal duplex ultrasound – may show renal artery stenosis, renal scarring or lesions
- Thyroid function test
- Sleep study
- 24 hour urine free cortisol
Investigations performed are mainly to rule out secondary causes of hypertension and to monitor over cardiovascular risk factors (ie. cholesterol)
End organ damage
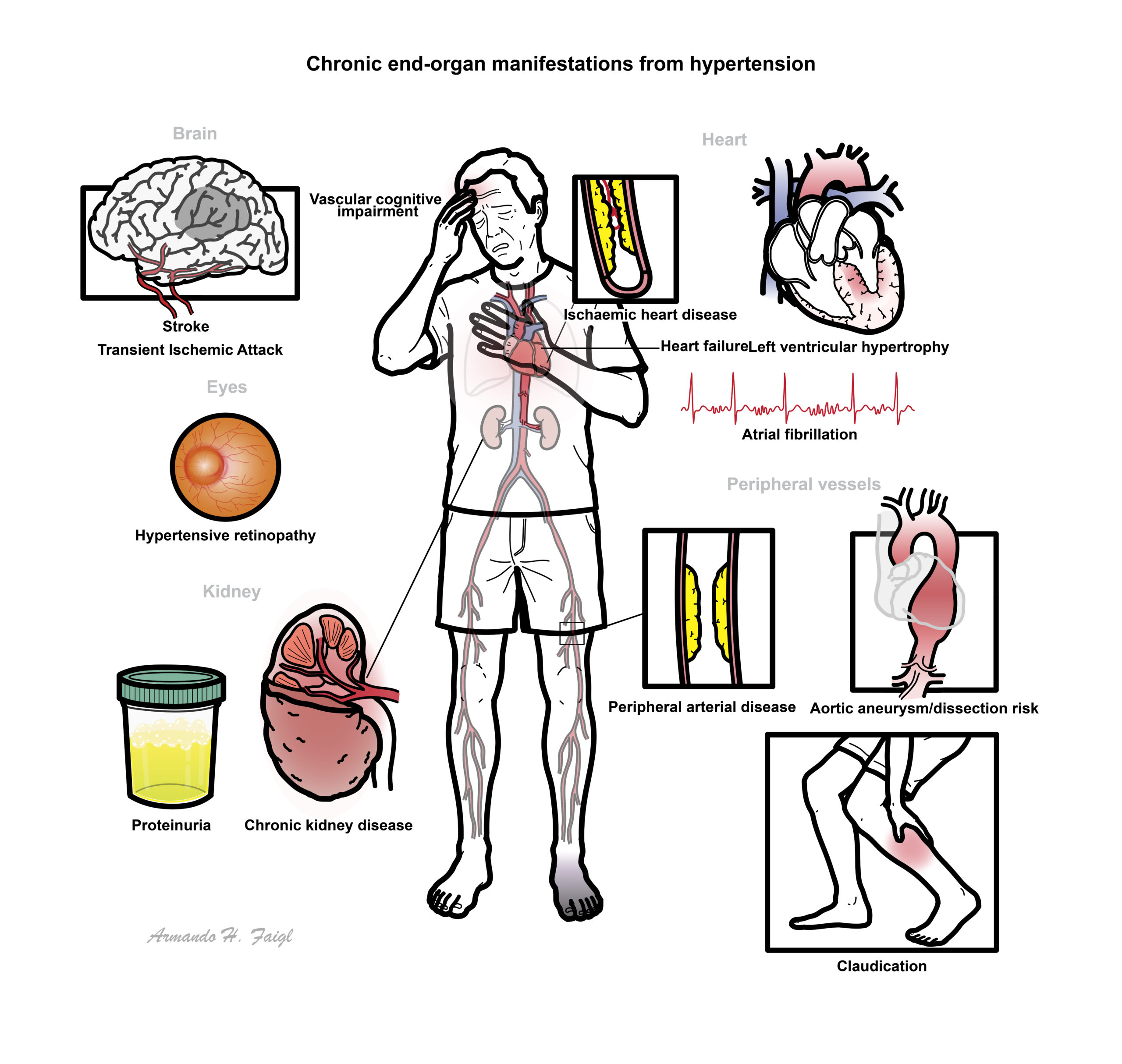
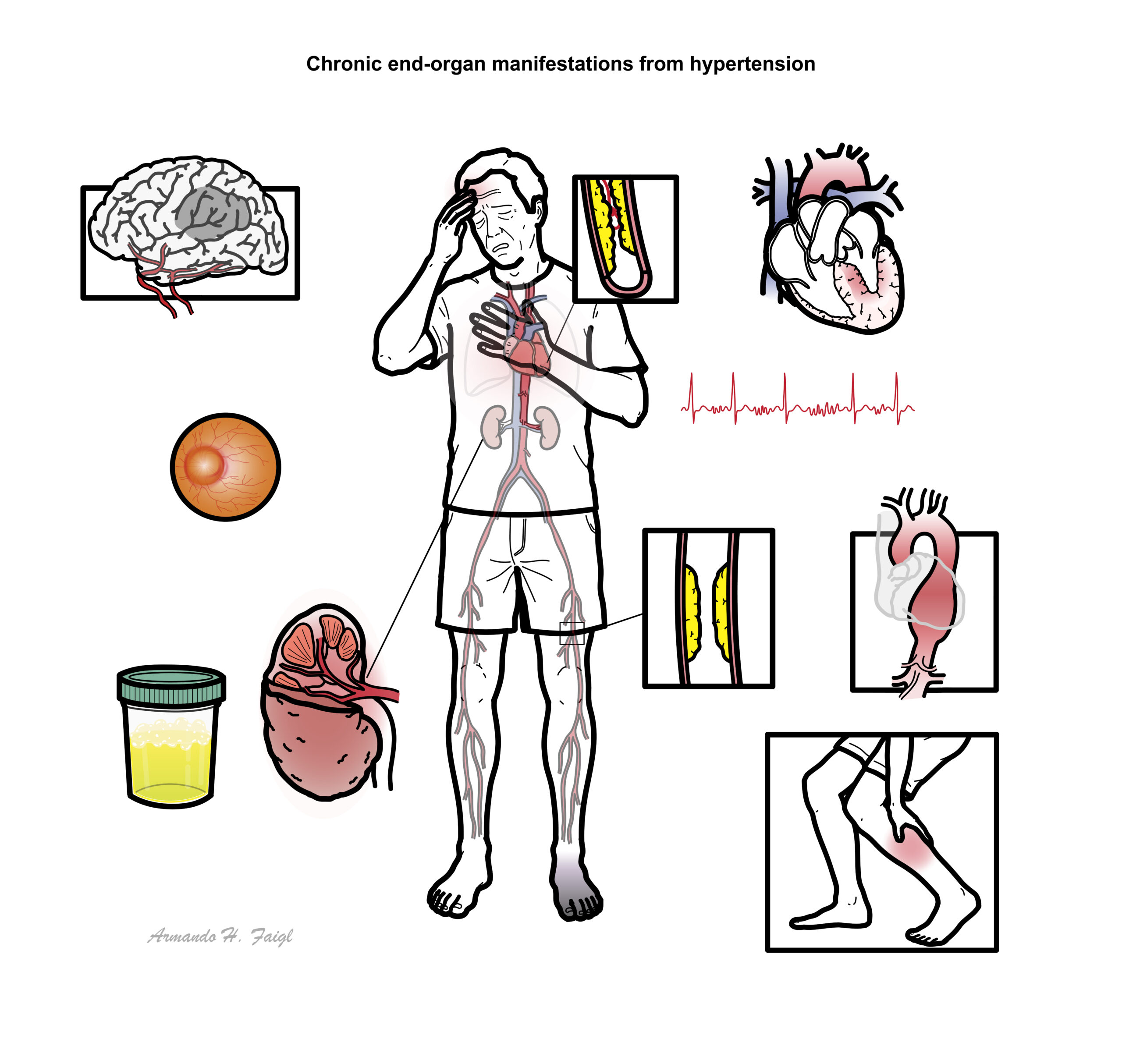
Cardiovascular disease
- Cardiac failure
- Left Ventricular hypertrophy
Cerebrovascular disease
- Transient ischaemic attack
- Cerebrovascular Attack
Renal failure
Retinopathy (Fundoscopy)
- Arteriolar narrowing
- Arteriolar venous nipping (nicking)
- Cotton wool spots
- Haemorrhages
- Papilloedema
| Hypertensive retinopathy classification | |
| I | Arteriolar constriction and narrowing |
| II | Severe narrowing and AV nipping |
| III | Features of grade I and II plus retinal haemorrhages, exudates, microaneurysms, cotton-wool spots |
| IV | All features above plus optic disc swelling +/- macular degeneration |
The aim of early diagnosis and treatment of hypertension is to lower overall cardiovascular risk and prevent cerebrovascular events. The effects of chronic hypertension on organ systems are referred to as target (end) organ damage.
Treatment
Management of chronic hypertension
- Education
- Sodium reduction
- Diet – high fruit and veg, whole grains, low sodium, low fat proteins
- Waist circumference reduction
- Increase physical activity – 30 min a day
- Limit alcohol consumption
- Smoking cessation
- Management of sleep apnoea
- Monitoring
Antihypertensive medication
Corner stone of managing primary hypertension is modifying poor life-style choices (ie. diet, smoking cessation). Antihypertensive medication are recommended for patient at high risk of cardiovascular disease and who have moderate-severe hypertension. Secondary causes of hypertension may require surgery and additional medications.
Management for end organ damage not discussed here
Follow up in 3 months then every 6 months there after
Antihypertensives first line Patients commonly require two or more drugs in combination to reach BP targets.
- Ace inhibitors/ARBs
- Calcium Channel Blockers
- Beta blockers are added as secondary
- Thiazide (typically for coexisting Congestive Heart Failure)
Initiate hypertensives immediately if hypertension grade III
The combination of an ACEI or ARB, a diuretic and a nonsteroidal anti-inflammatory drug – the triple whammy – can cause acute kidney failure.
Pharmacology
Ace inhibitors work by inhibiting the membrane bound enzyme ACE which usually converts Angiotensin I to Angiotensin II. Angiotensin II is a very strong sympathetomemetic increasing heart rate and contracitliy as well as being potent vasocontrictor. Side effect of ACE include dry cough, hyperkalaemia, angioedema and rash (+/- nausea, diarrhea, etc). Contraindications include chronic cough, allergy, pregnancy and renal failure. Alternative drug for ACE is ARBs which work just as effectively.
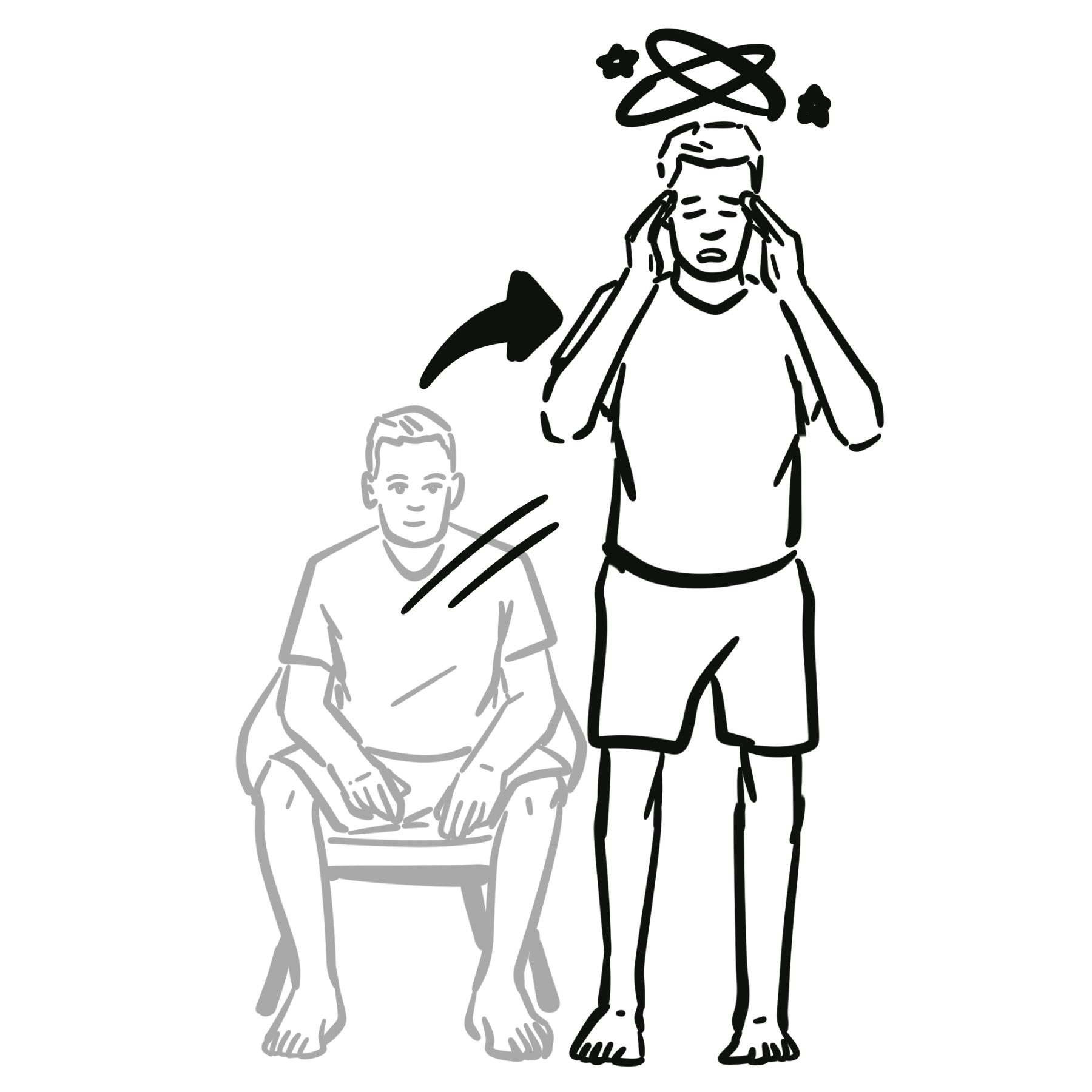
Common side effect of Beta blocker and Calcium channel blockers is orthostatic hypotension which is defined as a decrease in systolic blood pressure of 20 mm Hg or a decrease in diastolic blood pressure of 10 mm Hg within three minutes of standing when compared with blood pressure from the sitting or supine position.
Complications & Prognosis
- End organ damage
- Hypertensive retinopathy
- Non-compliance results in poorer prognosis
- Uncontrolled HTN is a major risk factor for the development of cardiac, vascular, renal, and cerebrovascular disease, morbidity, and mortality. However, even modest reductions in BP decrease morbidity and mortality
- In Diabetes reduction of BP to outcome is unclear.
Hypertensive Urgency and Emergency
Definition
Hypertensive Urgency is defined as BP ≥140/90 mmHg.
Hypertensive Emergency is elevated BP (usually systolic BP >210 mmHg and diastolic BP >130 mmHg) with rapid deterioration of vital organ function, resulting in symptoms such as encephalopathy, retinopathy, myocardial ischaemia, or renal failure.
Management of Hypertensive Urgency
- Nifedipine
- Prazocin
Hypertensive Emergency
Hypertensive emergency is elevated BP (usually systolic BP >210 mmHg and diastolic BP >130 mmHg) with rapid deterioration of vital organ function, resulting in symptoms such as encephalopathy, retinopathy, myocardial ischaemia, or renal failure. The absolute value of the BP is not as vital as the presence of acute end-organ damage.
Aetiology
- Undiagnosed and untreated essential hypertension
- Renal disease
- Pre-eclampsia
- Acute Pulmonary Oedema
- Other secondary hypertension causes
Management
- Bolus 1mg (up to 5mg)
- Metoprolol IV
- Hydralazine IV
- Antihypertensive Infusion
If untreated heart, neurological and renal impairment may ensue.
References
Therapeutic Guidelines Cardiology Version 6 2012
UpToDate
Best Practice
eTG – Australia




Members only discussions coming soon…