Overview Depressive disorders are typically characterised by persistent low mood, loss of interest and enjoyment, neurovegetative disturbance, and reduced energy, causing varying levels of social and occupational dysfunction. Depression is the leading cause of disability and premature death in 18-44 yo and is predicated to be the 2nd leading cause of disability in 2020. 20% of adults will have it at some point in their life, women are twice as likely. Depression will make up ~5-10% of people seen in primary care setting
| Definition Anhedonia: Loss of interest or pleasure in activities that were previously pleasurable Depression: Clinical Depression is an illness, a medical condition. It significantly affects the way someone feels, causing a persistent lowering of mood. Grief: Multifaceted response to loss, particularly to the loss of someone or something that has died, to which a bond or affection was formed. |
| Grief | Depression |
| There is an identifiable loss | A specific loss may or may not be identified |
| The person's focus is on the loss | The person's focus is on self |
| Fluctuating ability to feel pleasure | Inability to feel pleasure |
| Fluctuating physical symptoms | Prolonged and marked functional impairment |
| Closeness of others is usually comforting | Persistent isolation from other and self |
| Able to feel a wide range of emotions | Fixed emotions and feeling "stuck" |
| May express guilt over some aspects over loss | Generalised feelings of guilt |
| Thoughts of death are typically related to wanting to be reunited with the deceased loved one | Thoughts of death related to feeling worthless, undeserving of life or unable to cope with the pain |
Interview
History
| Mini State Examination (MSE) | Findings in Depression |
| Appearence and Behaviour | Desheveled, furrowing of brows, ↓rate of blinking, shoulder bent, head down, ↓gesture, ↓eye contant |
| Speech | Slow, long pauses, little spontaneous speech, low volume |
| Mood and affect | Low mood/misery (worse in morning), pessimistic about the present, hopelessness about future, guilt about the past, suicidal, dysphoric, blunt affect |
| Thought form and though content | Delusions common (especially persecutory) |
| Cognition | ↓attention, concentration and memory |
| Insight | variable |
| Perception | reduced intensity of normal perceptions. Occasionally auditory hallucinations |
Mental State Examination (ABCDEFGHIJ)
| Risk Factors |
| Age (onset peaks in late 20s) |
| Family history (3x risk with affected 1° relatives) |
| Personal history |
| Lower SES |
| Substance abuse |
| Adverse life events |
| Lack of confiding relationship |
| Physical illness |
| Remember Mneumonic SIG-E-CAPS for the signs and symptoms of Depression |
Non-specific symptoms of Depression
| Remember Rule out an underlying substance (eg, alcohol and cocaine withdrawal), medication (eg, antihypertensives, steroids), or medical condition causing depression (eg, hypothyroidism, multiple sclerosis), especially if the patient does not have a prior history of depression. |
Criteria for symptoms
Multifactorial
Changes in brain
| Remember The treatment that was successful for prior episodes of major depression has a higher likelihood of achieving remission in future episodes. |
Psychological therapy
Psychosocial treatments are first line treatments for mild depression. Usually psychotherapy is used in conjunction with pharmacotherapy.
Pharmacological therapy
None has been shown to be more effective then the other, so the choice depends on the adverse effects the patient can tolerate. SNRI are used first line because they generally have less side effects. When response to treatment is poor the diagnosis and compliance with treatment should be reassessed
| Think important to identify if patient also has manic episodes in the past, as antidepressent can induce a manic episode. |
| Remember Adults with major depressive disorder being treated with antidepressants should be observed for worsening depressed mood and suicidality, especially during the initial few months of a course of drug therapy, or at times of dose changes (either increases or decreases). |
| Pharmacology Selective serotonin reuptake inhibitors (SSRI) work by inhibiting the reuptake of serotonin from the synativ cleft thus increase serotonin effects on post synaptic neurons (causing good feels). Lower starting doses are often recommended and slowly increase and titrate accordingly. Side effects: Diarrhea, dizziness, dry mouth, fatigue, headache, sexual dysfunction, sweating, tremor, and weight gain are commonly reported. Nausea and vomiting are the most common reasons for discontinuation. Overdose of SSRI leads to serotonin syndrome (more info below) |
Moderate/severe depression:
Complications
| Remember Risk of suicide with SSRI (increase risk in young, risk decreases in old >25years) |
Prognosis
| Remember More than 50% of patients who have had one episode of major depression will have recurrent episodes. |
Overview Many experience what is known as postpartum blues, in which there is sadness, strong feelings of dependency, frequent crying spells, and dysphoria. This occurs in up to one in seven women.
Postpartum blues usually last for several days to a week. In rare cases, postpartum depression exceeds in both severity and length that is observed in postpartum blues and is characterized by suicidality and severely depressed feelings.
| Remember All women should be screened for depression during pregnancy and the postpartum period. |
Risk factors
Diagnosis -
Management
For first-time mothers, adolescent mothers, and mothers who have experienced a traumatic delivery, home health visits, telephone-based peer support, and psychotherapy may help prevent peripartum depression.
| Think Selective serotonin reuptake inhibitors are the most commonly used medications for depression but should not be used in conjunction with MAOIs. One medication should be discontinued for at least 5 weeks before the other is initiated to avoid serotonin syndrome. |
Serotonin syndrome is characterized by (in order of appearance) diarrhea, restlessness, extreme agitation, hyperreflexia, autonomic instability, myoclonus, seizures, hyperthermia, rigidity, delirium, coma, and death.
| Defintion Alternative medicine – refers to therapies used in place of conventional care Complementary medicine – therapies used in conjunction with mainstream medical therapies. These therapies do not replace medical regimens for serious medical problems but are offered to support the patient and family. Examples: massage, support groups, guided imagery, biofeedback, and hypnosis Folk medicine – refers to therapies provided by family or group members as part of a family or cultural tradition. Examples: using "cold" foods for "hot" illnesses, religious or ritual healing practices Integrative medicine – refers to the integration of CAM therapies into mainstream medical practice based upon evidence of safety and effectiveness within the context of relationship-based care promoting optimal health and wellbeing. Holistic medicine – refers to the care of the whole patient (eg, body, mind, emotions, spirit, and relationships) in the context of his or her values, beliefs, culture, and community. Examples of holistic medicine include promotion of literacy, screening for depression or alcohol use in family members, assessment of spirituality, and promotion of housecleaning to reduce allergic symptoms |
Classification of CAM
| Remember Patients and families may or may not discuss their use of CAM with their mainstream healthcare professionals, so it’s important to ask! |
CAM treatments used for depression
| Cytochrome p450 system The liver is responsible for the selective uptake, concentration, metabolism and excretion of the majority of drugs and toxins that are introduced to the body. Exogenous products are hepatically metabolized predominantly through two mechanisms: phase I and phase II reactions. Phase I reaction transform lipophilic molecules into more polar, hydrophilic molecules via oxidation, reduction, or hydrolysis. Phase II reactions often but not always involves a monooxygenase system in which CYP450 plays a key role. Cytochrome P450 enzymes can be inhibited or induced by drugs, resulting in clinically significant drug-drug interactions that can cause unanticipated adverse reactions or therapeutic failures. Interactions with warfarin, antidepressants, antiepileptic drugs, and statins often involve the cytochrome P450 enzymes. |
Overview Suicide is widespread across many age groups, and is associated with mental illness such as depression and other factors. Suicide is likely to be under-reported as deaths from suicide may be difficult to distinguish from accidental or intentional injury. It is important to note that suicide attempts are up to 20 times more frequent than completed suicide.
| Side note Suicide among medical practitioners is higher than other professional groups in many industrialised countries, especially among female doctors. Risk factors for suicide are the same as the general population, however there is greater knowledge about how succeed and the availability of methods which may contribute to relatively high suicide rates. |
| Definition Mental illness: A term referring to a group of conditions that significant affect how a person feels, thinks, behaves, and interacts. Mentally disordered person: A person (whether or not suffering from mental illness) whose behavior for the time being is so irrational as to justify a conclusion on reasonable grounds that temporary care, treatment, or control of the person is necessary |
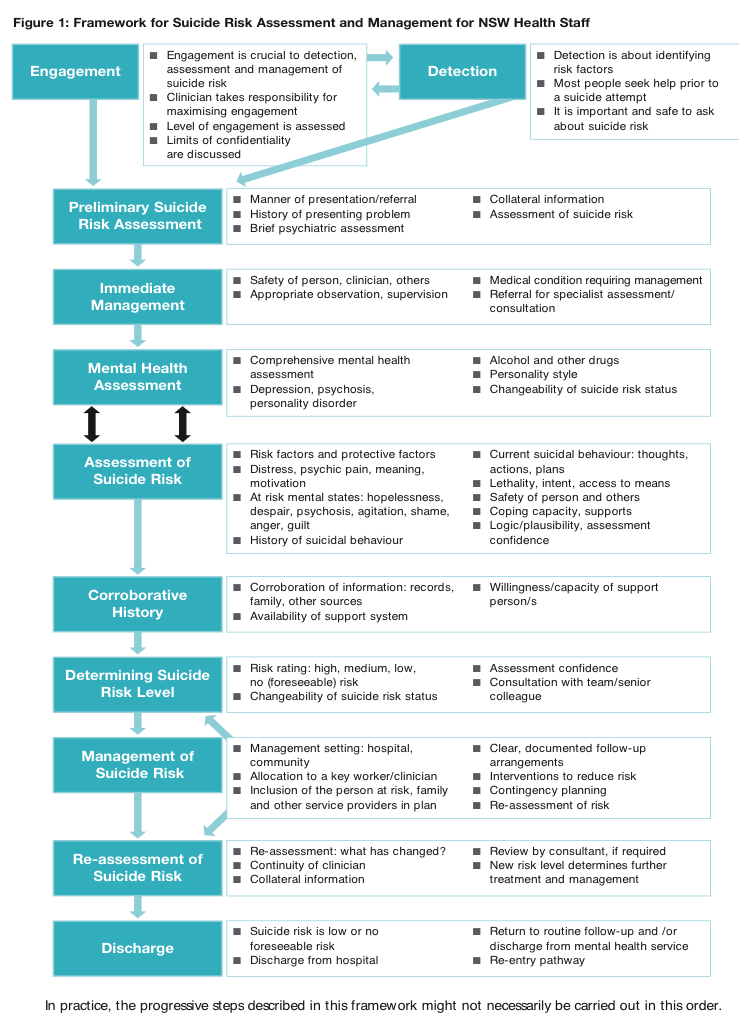
Suicide risk assessment – Important to complete when dealing with all patients who have mental health problems. The aim is to evaluate the likelihood of suicide attempt in the period of assessment.
Self-harm assessment (brief)
| RISK FACTORS AND PROTECTIVE FACTORS OF SUICIDE | ||
| Groups at Risk of suicide | Risk Factors | Protective Factors |
| History of attempt or self-harm | Male | Strong perceived social supports |
| History of mental illness | Between 25-44yo | Family cohesion |
| History of sexual or physical abuse/neglect | Older people | Peer group affiliation |
| Domestic violence | Living in rural areas | Good coping and problem solving skills |
| Substance abuse | Recent break-up | Positive values and beliefs |
| Physical illness | Sexual identity conflicts | Ability to seek and access help |
| Refugees, immigrants | Financial difficulties | |
| Homeless | Impending legal prosecutions | |
| Lack of support |
Involuntary treatment
Discharge following admission
DSM V categorise these as seperate disorders
Depressive Disorders