

Acute Heart Failure

Overview
Acute Heart Failure (AHF) is a life-threatening medical emergency defined as the rapid onset or sudden worsening of symptoms and signs of heart failure. It results from severe cardiac dysfunction leading to inadequate systemic cardiac output, elevated intracardiac pressures, or both. AHF can present either as de novo heart failure in a patient without prior cardiac disease or, far more commonly, as acute decompensation of chronic heart failure (ADHF).
The underlying pathophysiology is driven by acute hemodynamic instability, rapid neurohormonal activation, and acute volume overload or redistribution. Clinical management centers on immediate risk stratification based on hemodynamic profiling (evaluating congestion and perfusion status), stabilizing respiratory and cardiovascular function with oxygenation and non-invasive ventilation, rapidly relieving congestion with intravenous diuretics, and identifying and reversing acute precipitating triggers.
Definition
Acute Decompensated Heart Failure (ADHF): Rapid worsening of signs and symptoms in a patient with pre-existing chronic heart failure, accounting for over 75% of AHF admissions.
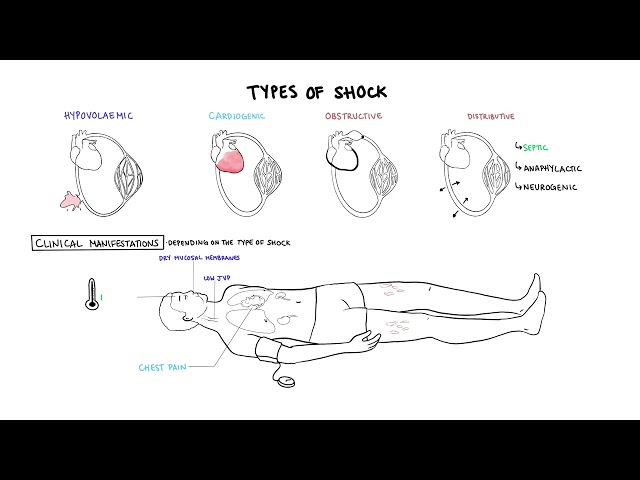
Cardiogenic Shock: A state of critical end-organ hypoperfusion caused by primary cardiac failure, defined as persistent hypotension (Systolic Blood Pressure < 90 mmHg or Mean Arterial Pressure drop > 30 mmHg) despite adequate filling pressure, accompanied by signs of tissue hypoperfusion (oliguria, cold extremities, altered mental state, elevated serum lactate).
Flash Pulmonary Edema: Sudden, dramatic onset of severe pulmonary congestion and respiratory distress caused by a rapid rise in left ventricular end-diastolic pressure, most commonly triggered by acute myocardial ischemia or a severe hypertensive crisis.
Warm vs. Cold / Wet vs. Dry Profiles: The Stevenson Hemodynamic Classification used at the bedside to categorize AHF patients based on perfusion (“Warm” vs. “Cold”) and congestion (“Wet” vs. “Dry”).
Cardiorenal Syndrome Type 1: Acute kidney injury resulting directly from acute cardiac decompensation and venous congestion.
Classification
AHF is classified by hemodynamic profile, clinical presentation, and left ventricular ejection fraction (LVEF).
Stevenson Hemodynamic Profiles (Bedside Classification)
- Warm and Wet (Most Common, ~80% of cases): Well-perfused but congested. Managed primarily with IV diuretics and vasodilators.
- Cold and Wet (~15% of cases): Hypoperfused and congested. High mortality; managed with IV diuretics, inotropes, and vasopressors if hypotensive.
- Cold and Dry (~5% of cases): Hypoperfused without clinical congestion. Caused by hypovolemia or right ventricular infarction; managed with cautious fluid challenge.
- Warm and Dry (Normal / Compensated): Well-perfused without congestion. Baseline state of compensated chronic heart failure.
Clinical Presentation Subtypes
- Acute Decompensated Heart Failure (ADHF): Gradual accumulation of fluid over days to weeks leading to systemic and pulmonary congestion.
- Acute Pulmonary Edema: Rapid intra-alveolar fluid accumulation presenting with severe dyspnoea, orthopnoea, and respiratory failure.
- Isolated Right Ventricular Failure: Characterized by systemic venous congestion (elevated JVP, hepatomegaly, peripheral edema) with low left-sided filling pressures.
- Cardiogenic Shock: Severe tissue hypoperfusion with refractory hypotension.
Left Ventricular Ejection Fraction (LVEF) Categories
- HFrEF (Heart Failure with Reduced Ejection Fraction): LVEF <= 40%.
- HFmrEF (Heart Failure with Mildly Reduced Ejection Fraction): LVEF 41–49%.
- HFpEF (Heart Failure with Preserved Ejection Fraction): LVEF >= 50%.
The Warm vs. Cold assessment determines the need for inotropes, while the Wet vs. Dry assessment determines the need for diuretics.
Aetiology & Risk Factors
Precipitating Triggers (The “CHAMPIT” Acronym)
Acute decompensation is frequently triggered by an acute event that must be rapidly identified and treated:
- C – Coronary Artery Syndrome: Acute myocardial infarction or unstable angina.
- H – Hypertensive Emergency: Severe surge in blood pressure causing acute LV afterload mismatch.
- A – Arrhythmia: Rapid atrial fibrillation, ventricular tachycardia, or severe bradycardia.
- M – Mechanical Cause: Acute valvular rupture (e.g., papillary muscle rupture causing acute mitral regurgitation), aortic dissection, or cardiac trauma.
- P – Pulmonary Embolism: Sudden increase in right ventricular afterload.
- I – Infection / Inflammation: Pneumonia, sepsis, or acute myocarditis.
- T – Tamponade / Toxins: Pericardial effusion with tamponade, medication non-adherence, or NSAID use.
Underlying Structural Risk Factors
- Ischemic Heart Disease: Prior myocardial infarction or chronic coronary artery disease (most common underlying cause).
- Hypertension: Long-standing uncontrolled systemic hypertension causing LV hypertrophy and diastolic dysfunction.
- Valvular Heart Disease: Aortic stenosis, mitral regurgitation, or prosthetic valve dysfunction.
- Cardiomyopathies: Dilated, hypertrophic, restrictive, or peripartum cardiomyopathy.
Always search for the CHAMPIT triggers during the initial emergency evaluation of AHF, as managing the underlying trigger is crucial to reversing acute decompensation.
Pathophysiology
- Hemodynamic Breakdown: Primary cardiac injury or increased afterload causes an abrupt rise in Left Ventricular End-Diastolic Pressure (LVEDP).
- Pulmonary Congestion: Pressure backs up into the left atrium and pulmonary veins. When pulmonary capillary hydrostatic pressure exceeds plasma oncotic pressure (~20–25 mmHg), protein-poor fluid leaks into the interstitial space and alveoli, causing acute pulmonary edema.
- Neurohormonal Cascade: Reduced forward stroke volume triggers intense activation of the Sympathetic Nervous System (SNS) and Renin-Angiotensin-Aldosterone System (RAAS), causing systemic vasoconstriction, increased afterload, and fluid retention, perpetuating a vicious cycle.
Acute pulmonary edema occurs when pulmonary capillary hydrostatic pressure rises rapidly above plasma oncotic pressure (~25 mmHg), forcing fluid into alveolar spaces.
Clinical Manifestations
Congestion (“Wet”) Manifestations
- Pulmonary Congestion:
- Severe Dyspnoea: Rapid-onset shortness of breath at rest.
- Orthopnoea: Inability to lie flat due to increased venous return; quantified by the number of pillows used.
- Paroxysmal Nocturnal Dyspnoea (PND): Sudden awakening from sleep gasping for air.
- Cough & Pink Frothy Sputum: Classic sign of severe alveolar flooding in acute pulmonary edema.
- Auscultatory Signs: Bilateral basilar crackles/rales (may extend to upper zones) and cardiac S3 gallop (pathognomonic for volume overload).
- Systemic Congestion:
- Elevated Jugular Venous Pressure (JVP): Prominent venous distension (> 3 cm above sternal angle) and positive hepatojugular reflux.
- Peripheral Oedema: Bilateral pitting lower limb edema, sacral edema (in bedridden patients), and ascites.
- Hepatomegaly & Right Upper Quadrant Pain: Due to acute hepatic capsular stretch from venous congestion.
Hypoperfusion (“Cold”) Manifestations
- Peripheral Perfusion: Cool, clammy extremities, livedo reticularis (mottling), and delayed capillary refill time (> 3 seconds).
- Hemodynamic Parameters: Narrow pulse pressure (difference between SBP and DBP < 25 mmHg) indicating low stroke volume.
- End-Organ Perfusion:
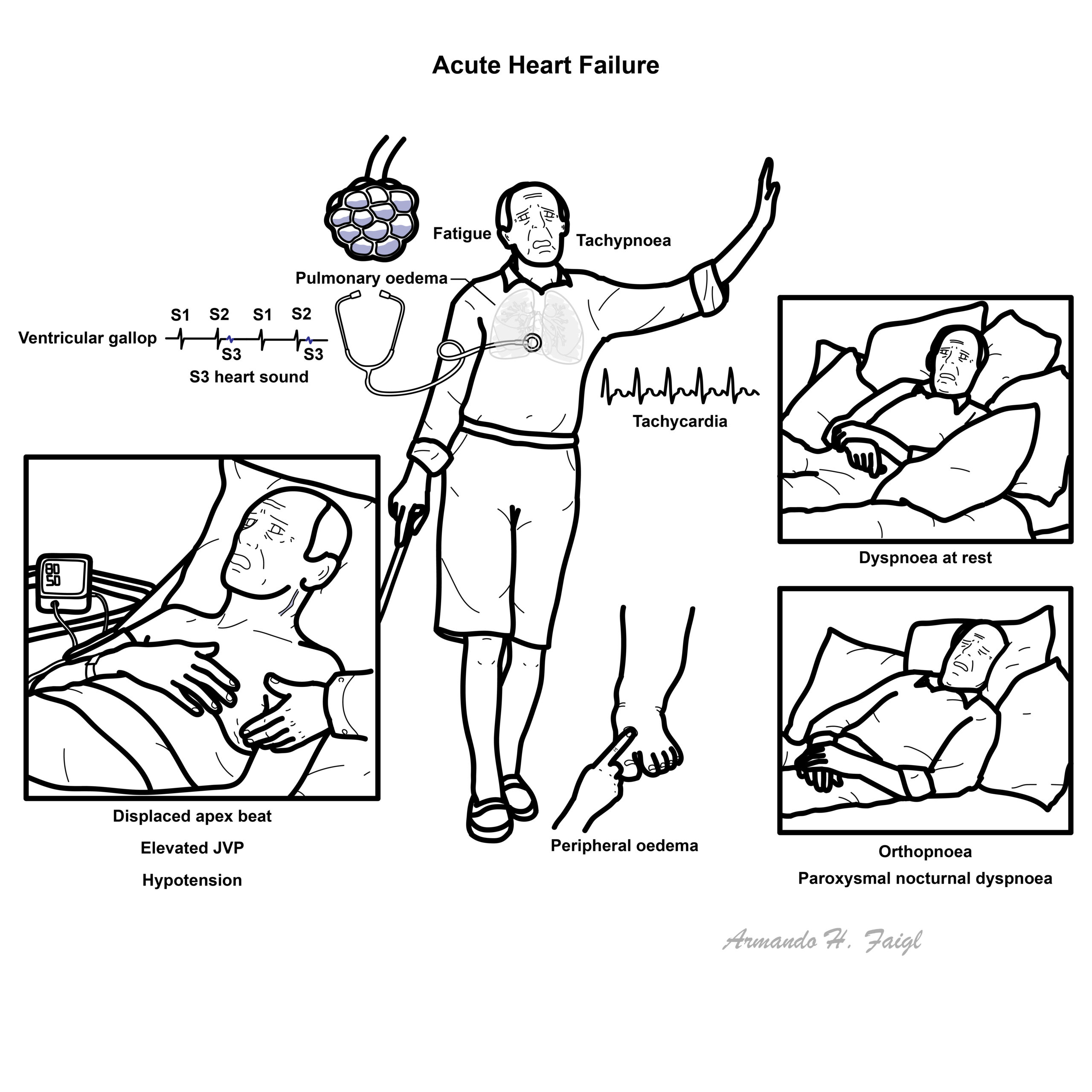
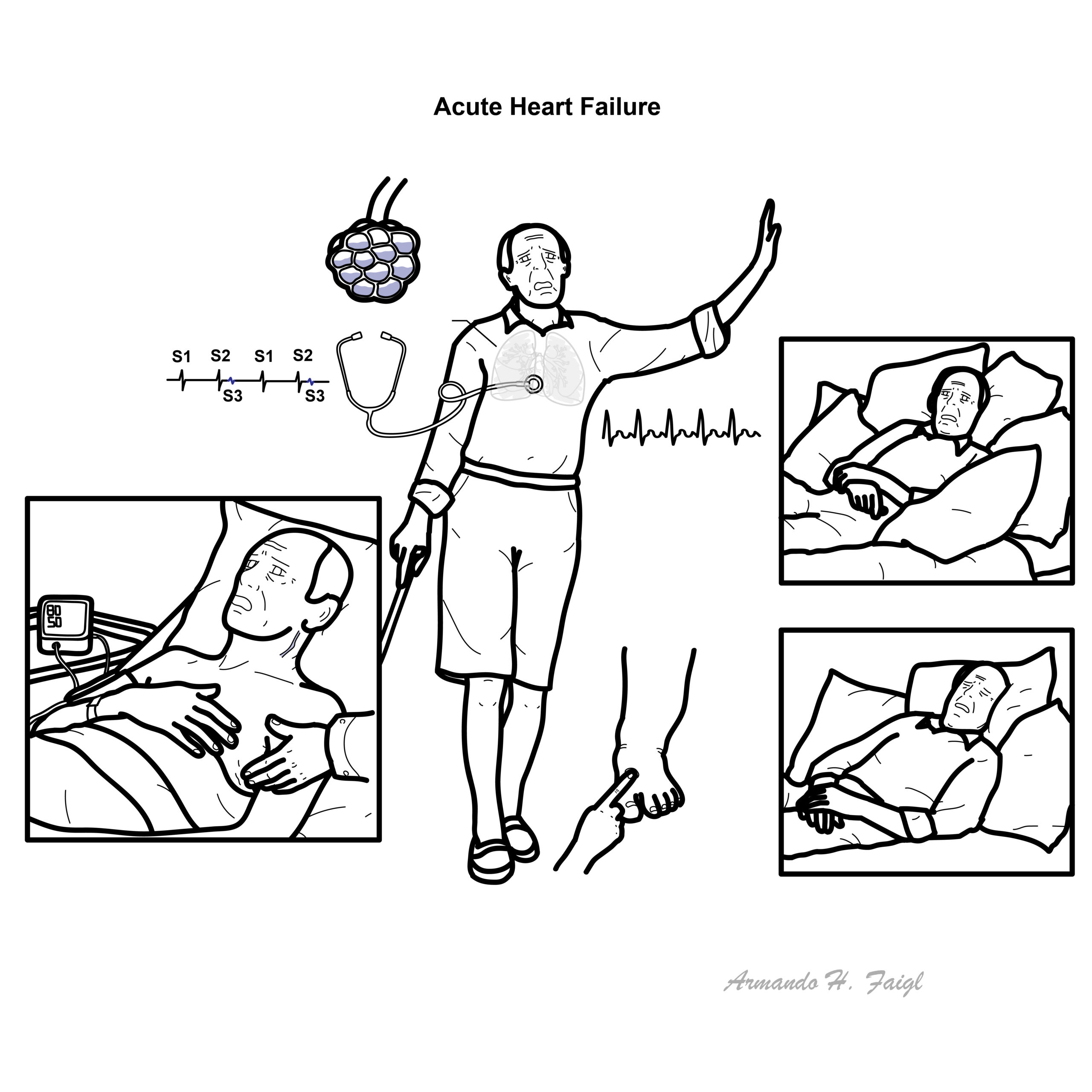
An S3 gallop combined with elevated JVP is highly specific for fluid overload and elevated left ventricular filling pressures in acute heart failure.
Diagnosis & Investigations
Bedside & Laboratory Investigations
- Natriuretic Peptides (BNP and NT-proBNP):
- BNP: < 100 pg/mL rules out AHF; > 400 pg/mL strongly supports AHF.
- NT-proBNP: < 300 pg/mL rules out AHF.
- Rule-in age-adjusted cut-offs: > 450 pg/mL (< 50 years), > 900 pg/mL (50–75 years), > 1800 pg/mL (> 75 years).
- Cardiac Troponin (I or T): Elevated in acute ischemia/MI and reflects ongoing cardiomyocyte injury.
- Renal & Metabolic Panel
- Arterial / Venous Blood Gas
Imaging & Diagnostics
- Electrocardiogram (ECG): Essential to identify acute ischemia, myocardial infarction, atrial fibrillation, or conduction blocks.
- Chest X-Ray (CXR): Classic features remembered by the ABCDE mnemonic:
- A – Alveolar Edema: “Bat-wing” or “butterfly” perihilar opacities.
- B – Kerley B Lines: Short, horizontal septal lines at lung bases indicating interstitial edema.
- C – Cardiomegaly: Cardiothoracic ratio > 50%.
- D – Dilated Upper Lobe Vessels: Cephalization of pulmonary blood flow.
- E – Pleural Effusions: Usually bilateral or right-sided.
- Transthoracic Echocardiogram (TTE): Gold standard for structural assessment; evaluates LVEF, regional wall motion abnormalities, valvular dysfunction, and estimated pulmonary artery pressures.
- Lung Ultrasound (POCUS): Rapid bedside test showing bilateral B-lines (“comet tails” >= 3 per intercostal space) representing interstitial lung water.
A normal BNP (< 100 pg/mL) or NT-proBNP (< 300 pg/mL) has an extremely high negative predictive value (> 95%) for ruling out acute heart failure in an acutely dyspneic patient.
Treatment
Immediate treatment focuses on restoring oxygenation, reducing cardiac filling pressures, and treating acute precipitating causes.
Immediate Respiratory Support
- Oxygen Therapy: Administer supplemental O2 only if SpO2 < 90% or PaO2 < 60 mmHg (routine normoxic oxygen causes vasoconstriction and increases afterload).
- Non-Invasive Ventilation (NIV – CPAP / BiPAP): First-line therapy for acute pulmonary edema with respiratory distress. Decreases venous return (preload), reduces afterload, opens collapsed alveoli, and reduces work of breathing.
Pharmacological Therapy by Hemodynamic Profile
- Warm and Wet (Congested with Adequate Perfusion)
- IV Loop Diuretics (First-Line): IV Furosemide (initial dose: 20–40 mg IV if diuretic-naive, or 1–2 times their oral daily dose if on chronic loop diuretics).
- IV Vasodilators: Nitroglycerin or Isosorbide Dinitrate IV infusion. Indicated in acute pulmonary edema or severe hypertensive AHF, provided Systolic Blood Pressure > 110 mmHg. Decreases preload and afterload rapidly.
- Cold and Wet (Congested with Hypoperfusion)
- Inotropic Agents: Dobutamine or Milrinone IV infusion to increase cardiac contractility and cardiac output.
- Vasopressors: Norepinephrine IV infusion if SBP < 90 mmHg or cardiogenic shock persists despite inotropes, to maintain coronary and end-organ perfusion pressure.
- IV Diuretics: Administered once blood pressure and perfusion are restored.
Chronic Guideline-Directed Medical Therapy (GDMT) Management
- Beta-Blockers: Do NOT start or up-titrate beta-blockers during acute decompensation. If the patient is already taking a beta-blocker, maintain a reduced dose unless the patient is in cardiogenic shock or severe bradycardia.
- ACEi / ARB / ARNI / SGLT2i: Continue or initiate once hemodynamically stable and volume overload is resolved.
Vasodilators (like IV Nitroglycerin) should NEVER be administered if Systolic Blood Pressure is < 110 mmHg. Beta-blockers should NEVER be initiated or up-titrated during acute decompensation.
Complications & Prognosis
- Cardiogenic Shock
- Cardiorenal Syndrome Type 1
- Acute Hepatic Congestion (“Shock Liver”)
- Malignant Arrhythmias
- Ranges from 4% to 10% for uncomplicated ADHF, but exceeds 40–50% if cardiogenic shock develops.
- High vulnerability period following discharge; 30-day readmission rates approach 20–25%.
- Poor prognosis is independently predicted by elevated admission blood urea nitrogen (BUN), elevated serum creatinine, low admission SBP (< 115 mmHg), troponin elevation, and hyponatremia (< 135 mmol/L).
The 30-day readmission rate for acute heart failure approaches 25%, making early post-discharge follow-up within 7–14 days essential.
References
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599-3726. doi:10.1093/eurheartj/ehab368
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18):e895-e1032. doi:10.1161/CIR.0000000000001063
- Kurmani S, Squire I. Acute Heart Failure: Definition, Classification and Epidemiology. Curr Heart Fail Rep. 2017;14(5):385-392. doi:10.1007/s11897-017-0351-y
- Here are 6 high-yield, exam-style questions covering clinical phenotypes, initial resuscitation, diagnostic markers, and etiology in Acute Heart Failure (AHF)—formatted in clean plain text so you can paste directly into WordPress.





Members only discussions coming soon…