Overview
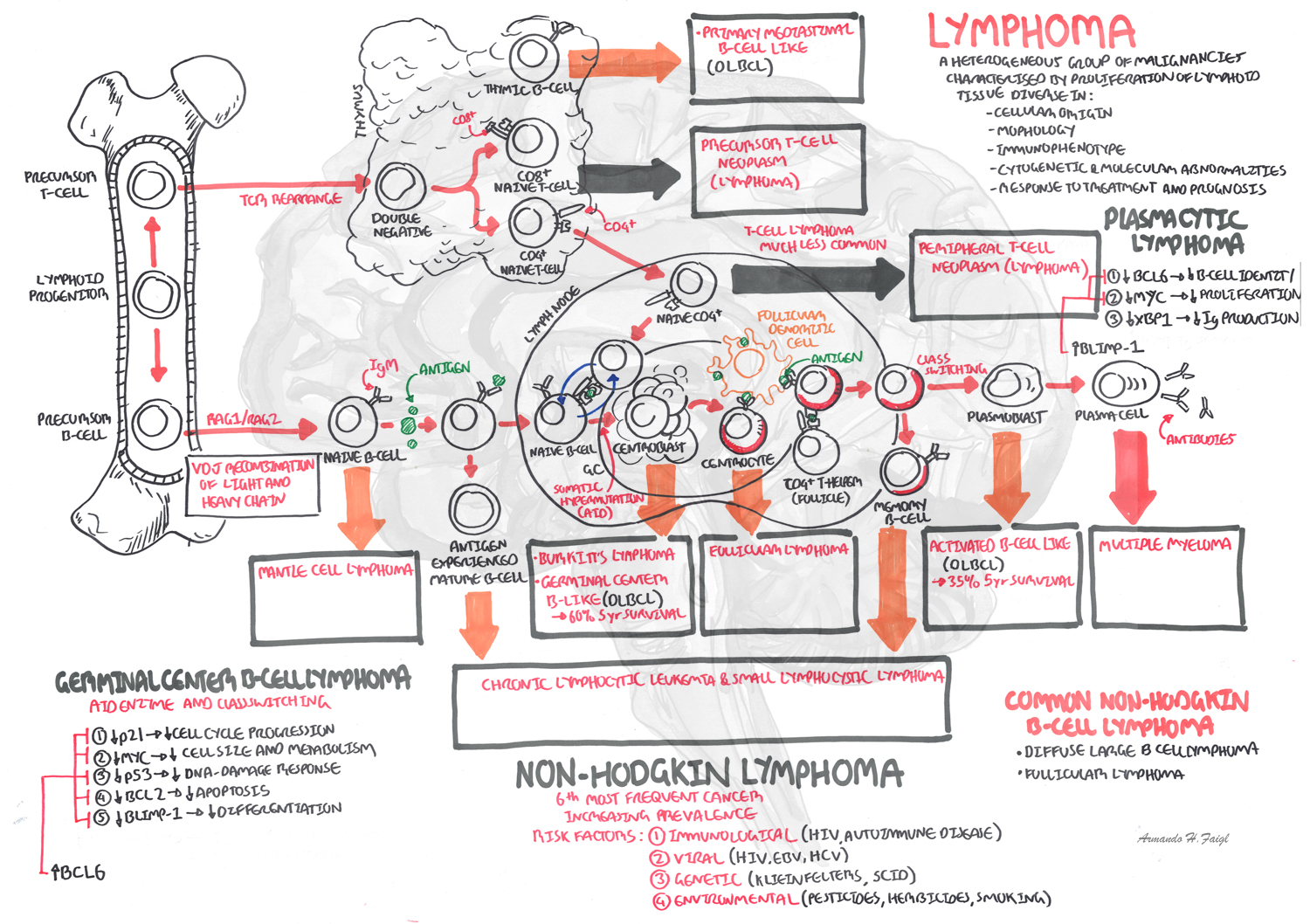
Lymphomas are derived from B and T lymphocytes or natural killer (NK) cells at varying stages of maturation. B cell lymphomas can arise at any stage of normal B cell development, but most are derived from cells that have been exposed to the germinal center reaction. T and natural killer (NK) cell lymphomas can arise at any stage of normal T or NK cell development. B cell lymphoma are more common.
Epidemiology
- Lymphoma is divided into Hodgkins and Non-Hodgkins Lymphoma (NHL)
- NHL accounts for 90% of all lymphomas
- The incidence of NHL increases with age.
- They are uncommon before age 50 years.
- The relative incidences of some of the most important types of NHL are:
- Diffuse large B-cell lymphoma (DLBCL)
- Follicular lymphoma (FL)
- The rest have 1% or lower incidence
Sign and Symptoms
- Night sweats
- Weight loss
- Fatigue
- Fever
- Lympadenopathy
- Splenomegaly
- Shortness of breath
- Cough
- Anaemia
Differential Diagnosis
- Hodgkins Lymphoma (bimodal age distribution at diagnosis -peaks at mid-20s and mid-60s, lymph node biopsy reveals Reed-Sternberg Cells)
- Acute Lymphoblastic Leukemia (acute onset, purpura, bleeding, and infection are key presenting symptoms.)
- Infectious mononucleosis (self-limiting condition with abrupt onset of symptoms; pharyngitis, rash and myalgias) - also known as the kissing disease
- Tuberculosis
- Rheumatoid Arthritis
- Systemic lupus erythematosus (SLE) (characteristic butterfly rash, photosensitivity, oral ulcers, arthritis)
| Acute lymphoblastic leukaemia tetrad: acute onset, purpura, bleeding, and infection |
Risk Factors
Immunological
- Autoimmune Diseases
- Immunodeficiency
Genetic
- Klienfelters Syndrome
- SCID
Viral
- Hepatitis C Virus (HCV)
- HIV
- EBV
Environmental
- Herbicides
- Pesticides
- Smoking
Investigations and Diagnosis
- Full blood count (thrombocytopenia, pancytopenia)
- Blood smear (nucleated red blood cells, giant platelets)
- Lymph node biopsy
- Bone marrow biopsy
- 30-50% of patients have involvement of bone
- LDH (elevated and is a indirect indication of proliferative rate of lymphoma)
- Erythrocyte sedimentation rate (elevated)
- CT scan (staging tool)
- Immunophenotype studies (Sub-classification of most forms of NHL)
- Flow cytometry -> on a single cell
- Immunohistochemistry -> on a tissue
Diagnosis
Lymph, Skin or Bone Marrow Biopsy can be used for diagnosis depending on the type of NHL. Imaging for monitoring progression (CT, PET)
Ann Arbor Staging System for NHL
- I: Single lymph node group
- II: Multiple lymph node groups on same side of diaphragm
- III: Multiple lymph node groups on both sides of diaphragm
- IV: Multiple extranodal sites
Pathophysiology
B and T cells have different stages of development. Accumulation of multiple genetic lesion affecting proto-oncogenes and Tumour Suppressor Genes (TGS) during stages of lymphocyte development leads to Lymphoma
B cell Lymphoma
- Majority of B cell lymphomas are derived from germinal center or post-germinal center B-cells
- Major genetic modifications occur during the normal germinal center reaction of B cells
- These changes (class-switch recombination and somatic hypermutation) are required for normal immune development, but also place the cell at risk of acquiring additional mutations that may be oncogenic
T cell Lymphoma
- Majority of T cell lymphomas are derived from post-thymic T cells.
- Gene rearrangement of T cell receptors (TCRs) is essential for the development of a highly diverse repertoire of TCRs required for an effective immune system, but also places the cell at risk for acquiring potentially oncogenic chromosomal translocations.
Treatment and Managment
Aggressive B-cell non-hodgkins Lymphoma
R-CHOP-21 (Rituximab, cyclophosphamide, doxorubicin, vincristine, prenisolone) +/- radiotherapy
Adjuncts
Methotrexate (CNS prophylaxis)
Mesna (high dose cyclophosphamide or ifosfamide are at risk of haemorrhagic cystitis)
Relapse on R-CHOP-21
R-ICE (Rituximab, phosphamide, carboplatin, etoposide)
Complications and Prognosis
Complications
- Chemotherapy side effects (Immunosuppression, hair loss, ulceration...)
- Radiation adverse effects (Inflammation, Secondary Leukaemia's)
- Tumour lysis syndrome
- Bone marrow transplant complication
Prognosis
In general, prognosis depends on the type of lymphoma, stage of disease, treatment, and comorbidities.
Worse prognosis is indicated by the following:
- B symptoms (weight loss, night sweats, and pyrexia)
- Lymphadenopathy
- Organomegaly
- Skin changes
Diffuse Large B-Cell Lymphoma (most common NHL)
- Stage I and II cure rate of up to 85%
- Stage III and IV cure rate of approximately 40%