Devastatingly disabling injury. Can be missed as ambulant patients may have an unstable vertebral injury. Up to 10% of unconscious patients have a significant vertebral injury. Most common cause of spinal injuries include MVA, Falls and pedestrian on roads. Ask yourself:
Complete vs incomplete spinal injury
Complete
Incomplete
Incomplete transverse spinal cord syndrome
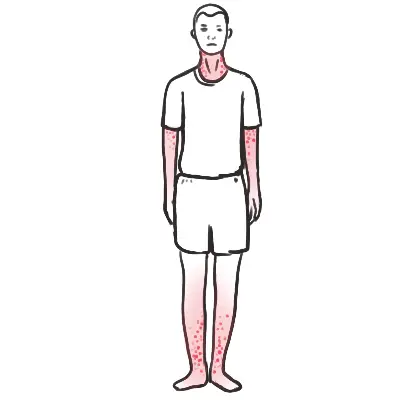
Central cord syndrome
Anterior cord syndrome
Posterior cord syndrome
Brown‐sequard syndrome – hemicord lesion
Effects of autonomic system
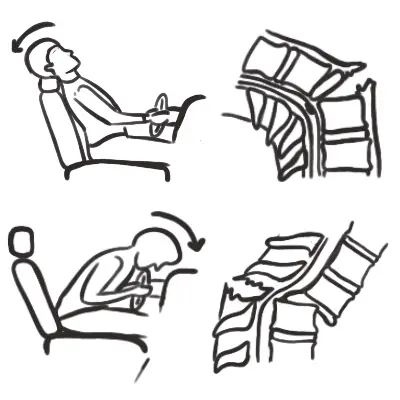
Cardiovascular‐ loss of vasomotor tone and any compensatory tachycardia
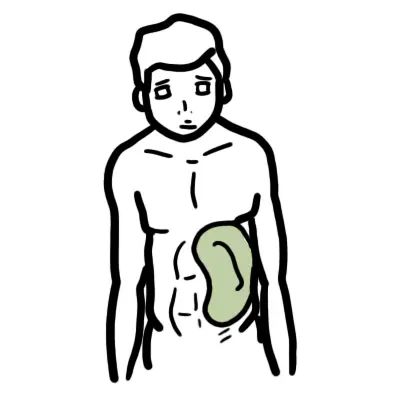
Gastrointestinal‐ passive aspiration due to sphincter tone loss, and paralytic ileus
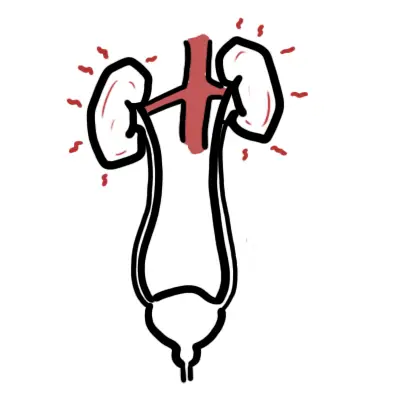
Urinary‐ bladder denervation resulting in over distension
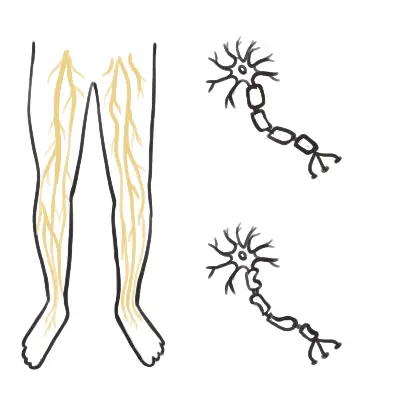
Thermoregulatory‐ loss of any compensatory mechanisms such as vasoconstriction and shivering and sweating
Spinal shock or neurogenic shock?
Spinal shock is transient cessation of all distal cord function lasting weeks to months‐ both somatic and autonomic function are lost (flaccid areflexia)
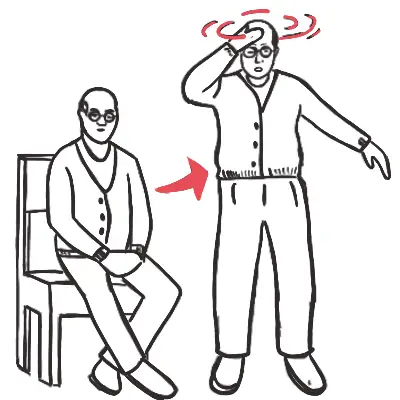
Neurogenic shock is autonomic loss (usually resulting from injury above T6) resulting in hypotension and bradycardia and peripheral dilation below the spinal lesion.
Facial, mandibular, or tracheal/laryngeal fractures
Inspect the spine for any gross deformities or ecchymosis. Palpate the spine noting any focal tenderness
Remember If the patient is able to communicate verbally, the airway is usually patent
Breathing – Look, listen, feel
Look at chest – is it rising?
Listen to breath sounds from mouth and auscultate chest
Feel for chest movement and breath
Identify any life-threatening conditions affecting thorax
Tension pneumothorax
Flail Chest
Massive haemothorax
Side note Ventilation may be reduced for a number of reasons, (1) diaphragm fatigue, (2) Progressively ascending spinal cord damage from primary damage or secondary ascending spinal cord oedema encroaching on C3-C5, (3) These same segments may be involved from primary injury and diaphragm may be partially paralysed and (4) Consequence of co-existing chest trauma.
Circulation
HR, BP, Capillary refill, skin colour
2 large IV insertion
Look for signs of shock or unstable rhythm
Hypotensive trauma victims should be considered as intravascularly volume depleted and bleeding until proven otherwise
Disability
GCS
Pupils – equal and reactive
Neurological examination – motor, sensory, reflex
Suspect C-spine injury until ruled out
Check for signs of ↑ICP – Cushing’s response (bradycardia, hypertension, irregular respirations)
Remember Cauda Equina Syndrome can occur with any spinal cord injury below T10 vertebrae. Look for incontinence, anterior thigh pain, quadriceps weakness, abnormal sacral sensation, decreased rectal tone, and variable reflexes.
Exposure/Environment
Increased risk of hyperthermia due to peripheral vasodilation
Look for other injuries
Fractures – Basilar skull fracture?
Scalp laceration
Burns
INVESTIGATIONS
Bedside
Laboratory
Imaging
Blood sugar
FBC
X-Ray – Neck, Thorax, Pelvis
ECG
EUC
Head CT scan (non-contrast)
VBG
Cross match
C-spine CT
FAST
Urinalysis
MRI – ligament injury suspected
Serum lactate
Management
Airway – Patent and Protected
Insertion of nasogastric tube important to minimise likelihood of aspiration
Ensure oxygen delivery to brain through intubation and prevent hypercarbia
Intubate if GCS < 9, patient is hypoxic, injury at or above C4
C-Spine support
Breathing – Look, listen, feel
Consider diaphragm issues (injury at C3, C4, C5)
Identify and treat life threatening chest injury
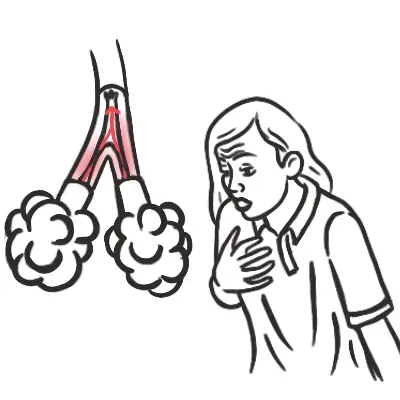
In the absence of major airway obstruction and flail chest, the presence of paradoxical breathing is considered highly suggestive of cervical spine injury
Circulation
Rule out hemorrhagic shock → maintain MAP >70
Look for signs of shock or unstable rhythm
If hypotensive – IV fluids
If seizure/risk – benzodiazepines, phenytoin, phenobarbital
Disability
GCS
Pupils – equal and reactive
Neurological examination – motor and sensory
Spinal immobilisation until spinal cord or unstable vertebral injury has been excluded on physical examination and investigations
Exposure/Environment
Increased risk of hyperthermia due to peripheral vasodilation








Discussion