Poisoning and Envenomation


“All things are poison and nothing is without poison, only the dose permits something not to be poisonous.”
–Paracelsus
Children are curious and explore their world with all their senses, including taste. As a result, the home and its surroundings can be a dangerous place when poisonous substances are inadvertently ingested – every year millions of calls are made to poison control centres when this happens and thousands of children are admitted to emergency departments. Poisoning exposure typically causes minor symptoms in young children; death is a relatively rare occurrence. The rate of fatal poisoning is highest for children under one year, with another slight peak around 15 years. Common poisoning agents in high-income countries include pharmaceuticals, household products (e.g. bleach, cleaning agents), pesticides, poisonous plants and bites from insects and animals.
| Remember If a child has collapsed, stopped breathing, is fitting or is suffering an anaphylactic reaction, CALL an ambulance. Do not ring the Poisons Information Centre in an emergency. |
| Important Questions |
| What was indigested? |
| When was the substance indigested |
| How much was indigested? |
| What is the weight of the child? |
| Poison | Antidote |
| Amphetamine | Esmolol, Labetalol |
| Benzodiazepine | Flumazenil |
| Beta-blocker | Glucagon, Isoprenaline, Adrenaline |
| Calcium Channel Blocker | Calcium chloride |
| Cyanide | Hydroxycobalamin with sodium thiosulfate |
| Digoxin | Digoxin Fab |
| Lead | If symptomatic Dimercaprol then calcium disodium edetate |
| Iron | Desferrioxamine |
| Opiates | Naloxone |
| Paracetamol | N-aceytlcysteine |
| Tetracycline Antidepressant | Sodium bicarbonate |
Ways to prevent poisoning:
Overview
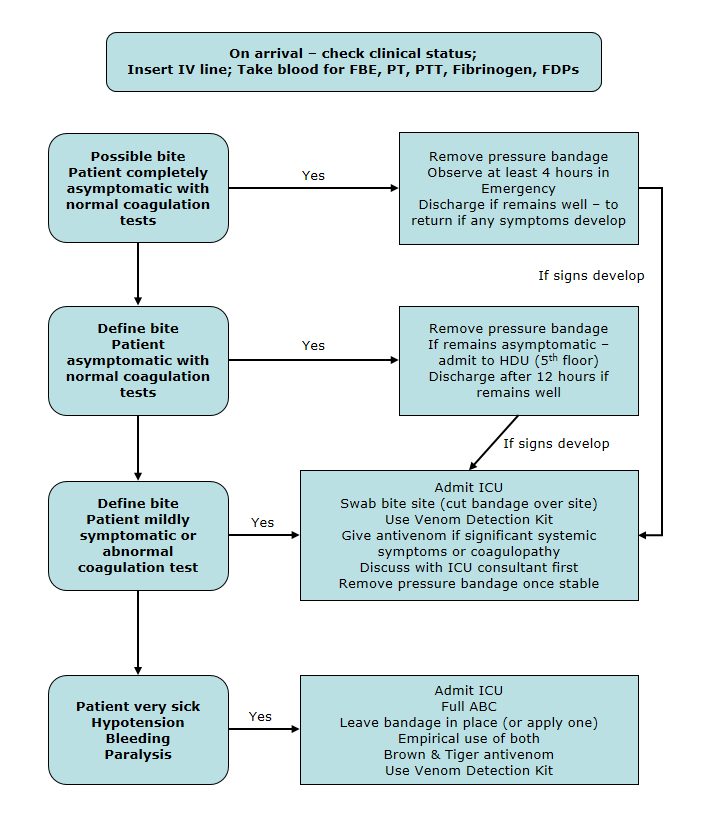
This section will mainly focus on snake bites. However, it is important to know that spider bites and jellyfish bites also exist. Venom from snakes may contain neurotoxins, procoagulants and rhadobmyolysins. Therefore, every snake bite should be regarded as potentially lethal.
| Definition Venom a poisonous substance secreted by animals such as snakes, spiders, and scorpions and typically injected into prey or aggressors by biting or stinging. Neurotoxins: a poison which acts on the nervous system. Procoagulants: inactive coagulation protein that becomes activated during the coagulation process to form a serine protease or cofactor and produce a fibrin clot. Rhadobmyolysins: substances which cause delayed destruction of skeletal muscle fibers. |
| Remember DO NOT remove bandage until in a centre with full treatment facilities, including available anti-venom and access to laboratory testing. Do not wash or clean the bite site in any way. |
| Spider envenomation Spider bite is common, but most species cause minimal or no effects. Spider identification is problematic and the clinician is better off recognising the ‘toxindrome’ (ie. signs and symptoms associated with medically significant spider bite) than attempting to identify the spider responsible for the bite. The two main types of spider venom are: neurotoxic (affects the nervous system) and cytotoxic or necrotic (causing damage to tissue). Always consider spider bite in the differential diagnosis of unexplained autonomic and neurological dysfunction, particularly in children. In Australia, skin ulceration is more likely to be an infective, inflammatory or traumatic cause than a case of necrotising arachnidism. |




Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion