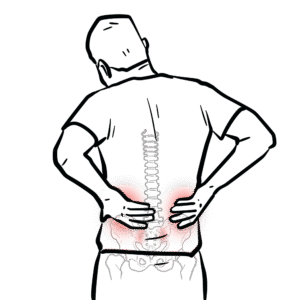
Devastatingly disabling injury. Can be missed as ambulant patients may have an unstable vertebral injury. Up to 10% of unconscious patients have a significant vertebral injury. Most common cause of spinal injuries include MVA, Falls and pedestrian on roads. Ask yourself:
Complete vs incomplete spinal injury
Complete
Incomplete
Incomplete transverse spinal cord syndrome
Central cord syndrome
Anterior cord syndrome
Posterior cord syndrome
Brown‐sequard syndrome – hemicord lesion
Effects of autonomic system
Cardiovascular‐ loss of vasomotor tone and any compensatory tachycardia
Gastrointestinal‐ passive aspiration due to sphincter tone loss, and paralytic ileus
Urinary‐ bladder denervation resulting in over distension
Thermoregulatory‐ loss of any compensatory mechanisms such as vasoconstriction and shivering and sweating
Spinal shock is transient cessation of all distal cord function lasting weeks to months‐ both somatic and autonomic function are lost (flaccid areflexia)
Neurogenic shock is autonomic loss (usually resulting from injury above T6) resulting in hypotension and bradycardia and peripheral dilation below the spinal lesion.
Side note Ventilation may be reduced for a number of reasons, (1) diaphragm fatigue, (2) Progressively ascending spinal cord damage from primary damage or secondary ascending spinal cord oedema encroaching on C3-C5, (3) These same segments may be involved from primary injury and diaphragm may be partially paralysed and (4) Consequence of co-existing chest trauma.
Circulation
HR, BP, Capillary refill, skin colour
2 large IV insertion
Look for signs of shock or unstable rhythm
Hypotensive trauma victims should be considered as intravascularly volume depleted and bleeding until proven otherwise
Insertion of nasogastric tube important to minimise likelihood of aspiration
Ensure oxygen delivery to brain through intubation and prevent hypercarbia
Intubate if GCS < 9, patient is hypoxic, injury at or above C4
C-Spine support
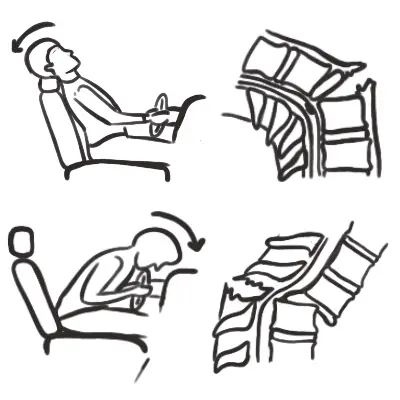
Breathing – Look, listen, feel
Consider diaphragm issues (injury at C3, C4, C5)
Identify and treat life threatening chest injury
In the absence of major airway obstruction and flail chest, the presence of paradoxical breathing is considered highly suggestive of cervical spine injury












Discussion