Remember
Wounds require tetanus prophylaxis and broad spectrum antibiotic if significant risk of contamination, or debridement of necrotic tissue.
History
Likely foreign body
Which eye
Mechanism
Protective eye wear?
Previous eye trauma – reduced structural integrity
When did it happen?
Contact lens wearer
What are the symptoms?
Photophobia
Discharge and type
Side note Small projectiles at high velocities increase the likelihood of penetrating trauma. Symptoms include loss of vision, pain on movement and diplopia.
Features requiring urgent referral Contact lens wearer Previous eye surgery or refractive surgery Decreased vision Severe pain Nausea and vomiting Cloudy or opaque cornea Dendritic ulcer Hypopyon (pus in the anterior chamber) Nonreactive pupils or RAPD Ocular trauma Persisting or worsening symptoms Chemical to eye
Blunt trauma
Types
Closed globe injury
Ruptured globe
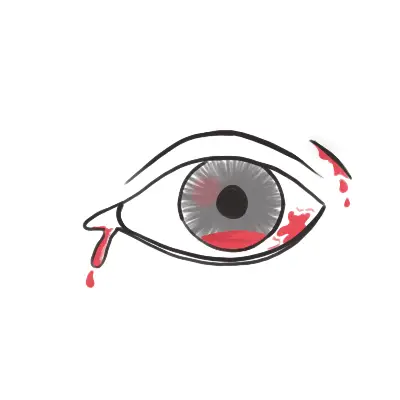
Signs
Haemorrhage
Hyphaema
Vitreous
Retina → retinal detachment
Vision changes
Iris damage
Lens damaged or dislocated
Angle of eye drainage damage
Investigate: CT scan for orbital wall fracture
Management : Topical antibiotics and suture eye lid lacerations and urgent referral
Signs of an inferior blowout fracture Ecchymosis/oedema Diplopia A recessed eye Defective eye movement Ipsilateral nose bleed Diminished sensation over the distribution of the infraorbital nerve
Penetrating trauma
Prolapse of the intraocular contents and irreversible damage can occur
Signs:
Distorted pupil
Cataract
Prolapsed black uveal tissue on the ocular surface
Vitreous haemorrhage
Dilate pupil and search for intraocular foreign body
Radiograph with eye in up and down gaze
Apply shield and transfer to eye department
All penetrating eye injuries need immediate referral
Management:
Nil by mouth
Strict bed rest
Analgesia /antiemeticCT Shield (not pad)
Tetanus status
Broad spectrum antibiotics
Corneal foreign body
Any foreign body penetration of the cornea or retained foreign body will require urgent referral to ophthalmologist – immediate consult by phone
Management removing corneal foreign body
Topical anaesthetic
Slit lamp and remove body
Cotton bud
Fine needle
Motorised dental burr
Use fluorescein to assess and measure the size of epithelial defect
Topical antibiotics and cycloplegic agent
Refer to ophthalmologist if body not removed and symptoms worsen
Chemical Burns Management
Instil local anaesthetic drops to affected eye/eyes.
Commence irrigation with 1 litre of a neutral solution, eg N/Saline (0.9%), Hartmann’s.
Evert the eyelid and clear the eye of any debris / foreign body that may be present by sweeping the conjunctival fornices with a moistened cotton bud.
Continue to irrigate, aiming for a continuous irrigation with giving set regulator fully open.
If using a Morgan Lens, carefully insert the device now.
Review the patient’s pain level every 10 minutes and instil another drop of local anaesthetic as required.
After one litre of irrigation, review.
If using a Morgan Lens, remove the device prior to review.
Wait 5 minutes after ceasing the irrigation luid then check pH. Acceptable pH range 6.5-8.5.
Consult with the senior medical oficer and recommence irrigation if necessary.
Severe burns will usually require continuous irrigation for at least 30 minutes
Immediate referral
Alkali Acidic Lime Toilet cleaner Mortor & plaster Car battery fluid Drain cleaner Pool cleaner Oven cleaner Ammonia










Discussion