Hypertension

Hypertension can be divided into primary (essential) and secondary hypertension (a result of an underlying condition, ie. renal artery stenosis). It is important to identify wether this is an underlying cause of the hypertension based on history, risk factors and by ordering appropriate tests. Untreated, undiagnosed and poor compliancy can result in and hasten end organ damage. Lifestyle changes is the corner stone of treatment.
Hypertension is defined as BP ≥140/90 mmHg. Hypertension can be divided into Primary or Secondary. The main goal of treatment is to decrease the risk of mortality and of cardiovascular and renal morbidity.
| Classification | Systole |
| Normal | 120-129 |
| High-normal | 130-139 |
| Hypertension Grade I | 140-159 |
| Hypertension Grade II | 160-179 |
| Hypertension Grade III | >180 |
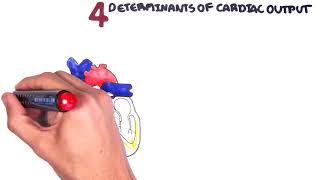
The mean arterial pressure (MAP) is a term used in medicine to describe an average blood pressure in an individual. MAP is a product of cardiac output and the total peripheral resistance.
Epidemiology
Risk Factors for hypertension are essentially the same for other cardiovascular diseases.
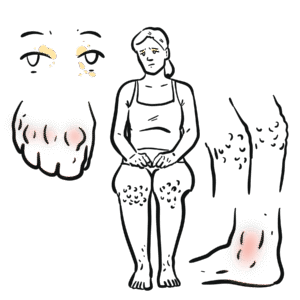
Hypertension is a common disorder that affects a large proportion of the community. It is usually asymptomatic and is detected on routine examination or after the occurrence of a complication such as a heart attack or stroke. It is often referred to as the silent killer.
Several things can cause bias to the hypertension readings (White coat hypertension). In the clinic, usually the 1st measurement is disregarded and the average of the second and third readings are taken.
Primary hypertension
This is the most common situation, when no underlying cause can be found to account for raised blood pressure.
Secondary hypertension
In a minority of cases, an underlying, often reversible cause can be found.
Vascular
Renal artery stenosis should be suspected if BP is unexpectedly low or kidney function deteriorates in patients taking an ACEI or ARB.
Kidneys
Endocrine
Toxic causes
Pseudo-hypertension
There are many causes of hypertension. Primary hypertension is mainly a result of lifestyle and genetics. Secondary hypertension is cause by an underlying, often reversible condition (ie. renal artery stenosis, medication)
Investigations
Although in the majority of patients hypertension is primary/essential, there are certain features that may lead to a suspicion of an underlying cause (secondary hypertension):Young patient (<40 years)Rapid onset of hypertensionSudden change in blood pressure readings when previously well controlled on a particular therapyResistant hypertension that is unresponsive to pharmacological therapies.
Investigations performed are mainly to rule out secondary causes of hypertension and to monitor over cardiovascular risk factors (ie. cholesterol)
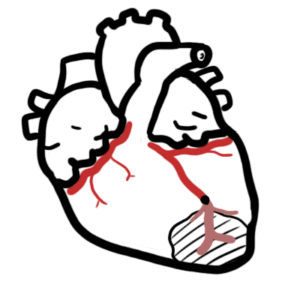
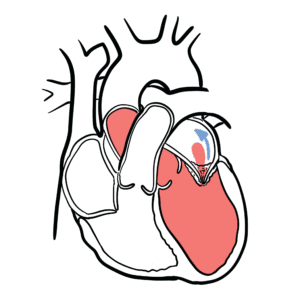
Cardiovascular disease
Cerebrovascular disease
Renal failure
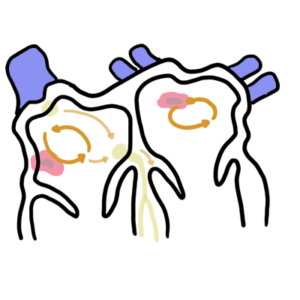
Retinopathy (Fundoscopy)
| Hypertensive retinopathy classification | |
| I | Arteriolar constriction and narrowing |
| II | Severe narrowing and AV nipping |
| III | Features of grade I and II plus retinal haemorrhages, exudates, microaneurysms, cotton-wool spots |
| IV | All features above plus optic disc swelling +/- macular degeneration |
The aim of early diagnosis and treatment of hypertension is to lower overall cardiovascular risk and prevent cerebrovascular events. The effects of chronic hypertension on organ systems are referred to as target (end) organ damage.
Management of chronic hypertension
Antihypertensive medication
Corner stone of managing primary hypertension is modifying poor life-style choices (ie. diet, smoking cessation). Antihypertensive medication are recommended for patient at high risk of cardiovascular disease and who have moderate-severe hypertension. Secondary causes of hypertension may require surgery and additional medications.
Management for end organ damage not discussed here
Follow up in 3 months then every 6 months there after
Antihypertensives first line Patients commonly require two or more drugs in combination to reach BP targets.
Initiate hypertensives immediately if hypertension grade III
The combination of an ACEI or ARB, a diuretic and a nonsteroidal anti-inflammatory drug – the triple whammy – can cause acute kidney failure.
Ace inhibitors work by inhibiting the membrane bound enzyme ACE which usually converts Angiotensin I to Angiotensin II. Angiotensin II is a very strong sympathetomemetic increasing heart rate and contracitliy as well as being potent vasocontrictor. Side effect of ACE include dry cough, hyperkalaemia, angioedema and rash (+/- nausea, diarrhea, etc). Contraindications include chronic cough, allergy, pregnancy and renal failure. Alternative drug for ACE is ARBs which work just as effectively.
Common side effect of Beta blocker and Calcium channel blockers is orthostatic hypotension which is defined as a decrease in systolic blood pressure of 20 mm Hg or a decrease in diastolic blood pressure of 10 mm Hg within three minutes of standing when compared with blood pressure from the sitting or supine position.
Complications
Prognosis
Hypertensive Urgency is defined as BP ≥140/90 mmHg.
Hypertensive Emergency is elevated BP (usually systolic BP >210 mmHg and diastolic BP >130 mmHg) with rapid deterioration of vital organ function, resulting in symptoms such as encephalopathy, retinopathy, myocardial ischaemia, or renal failure.
Management of Hypertensive Urgency
Hypertensive Emergency
Hypertensive emergency is elevated BP (usually systolic BP >210 mmHg and diastolic BP >130 mmHg) with rapid deterioration of vital organ function, resulting in symptoms such as encephalopathy, retinopathy, myocardial ischaemia, or renal failure. The absolute value of the BP is not as vital as the presence of acute end-organ damage.
Aetiology
Management
If untreated heart, neurological and renal impairment may ensue.
Therapeutic Guidelines Cardiology Version 6 2012
UpToDate
Best Practice
eTG – Australia







Please confirm you want to block this member.
You will no longer be able to:
Please allow a few minutes for this process to complete.
Discussion